Download
1 / 1
10 likes | 69 Views
No. 080. Management of local recurrences in the irradiated bladder: A systematic review. Nikhil Sapre 1 , Paul Anderson 1 , Farshad Foroudi, 1,2 1 Departments of Urology and Surgery, Royal Melbourne Hospital, University of Melbourne, VIC, Australia.

E N D
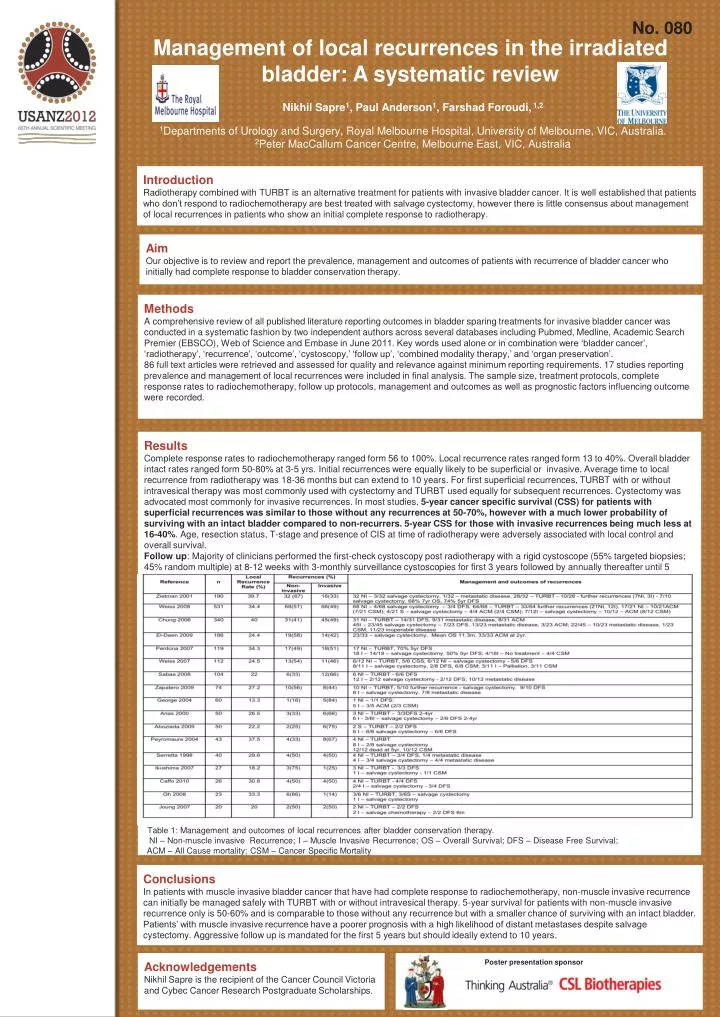
No. 080 Management of local recurrences in the irradiated bladder: A systematic review Nikhil Sapre1, Paul Anderson1, Farshad Foroudi, 1,2 1Departments of Urology and Surgery, Royal Melbourne Hospital, University of Melbourne, VIC, Australia. 2Peter MacCallum Cancer Centre, Melbourne East, VIC, Australia • Introduction • Radiotherapy combined with TURBT is an alternative treatment for patients with invasive bladder cancer. It is well established that patients who don’t respond to radiochemotherapy are best treated with salvage cystectomy, however there is little consensus about management of local recurrences in patients who show an initial complete response to radiotherapy. • Aim • Our objective is to review and report the prevalence, management and outcomes of patients with recurrence of bladder cancer who initially had complete response to bladder conservation therapy. • Methods • A comprehensive review of all published literature reporting outcomes in bladder sparing treatments for invasive bladder cancer was conducted in a systematic fashion by two independent authors across several databases including Pubmed, Medline, Academic Search Premier (EBSCO), Web of Science and Embase in June 2011. Key words used alone or in combination were ‘bladder cancer’, ‘radiotherapy’, ‘recurrence’, ‘outcome’, ‘cystoscopy,’ ‘follow up’, ‘combined modality therapy,’ and ‘organ preservation’. • 86 full text articles were retrieved and assessed for quality and relevance against minimum reporting requirements. 17 studies reporting prevalence and management of local recurrences were included in final analysis. The sample size, treatment protocols, complete response rates to radiochemotherapy, follow up protocols, management and outcomes as well as prognostic factors influencing outcome were recorded. • Results • Complete response rates to radiochemotherapy ranged form 56 to 100%. Local recurrence rates ranged form 13 to 40%. Overall bladder intact rates ranged form 50-80% at 3-5 yrs. Initial recurrences were equally likely to be superficial or invasive. Average time to local recurrence from radiotherapy was 18-36 months but can extend to 10 years. For first superficial recurrences, TURBT with or without intravesical therapy was most commonly used with cystectomy and TURBT used equally for subsequent recurrences. Cystectomy was advocated most commonly for invasive recurrences. In most studies, 5-year cancer specific survival (CSS) for patients with superficial recurrences was similar to those without any recurrences at 50-70%, however with a much lower probability of surviving with an intact bladder compared to non-recurrers. 5-year CSS for those with invasive recurrences being much less at 16-40%. Age, resection status, T-stage and presence of CIS at time of radiotherapy were adversely associated with local control and overall survival. • Follow up: Majority of clinicians performed the first-check cystoscopy post radiotherapy with a rigid cystoscope (55% targeted biopsies; 45% random multiple) at 8-12 weeks with 3-monthly surveillance cystoscopies for first 3 years followed by annually thereafter until 5 years. Table 1: Management and outcomes of local recurrences after bladder conservation therapy. NI – Non-muscle invasive Recurrence; I – Muscle Invasive Recurrence; OS – Overall Survival; DFS – Disease Free Survival; ACM – All Cause mortality; CSM – Cancer Specific Mortality Conclusions In patients with muscle invasive bladder cancer that have had complete response to radiochemotherapy, non-muscle invasive recurrence can initially be managed safely with TURBT with or without intravesical therapy. 5-year survival for patients with non-muscle invasive recurrence only is 50-60% and is comparable to those without any recurrence but with a smaller chance of surviving with an intact bladder. Patients’ with muscle invasive recurrence have a poorer prognosis with a high likelihood of distant metastases despite salvage cystectomy. Aggressive follow up is mandated for the first 5 years but should ideally extend to 10 years. Acknowledgements Nikhil Sapre is the recipient of the Cancer Council Victoria and Cybec Cancer Research Postgraduate Scholarships. Poster presentation sponsor