Download
1 / 73
940 likes | 3.04k Views
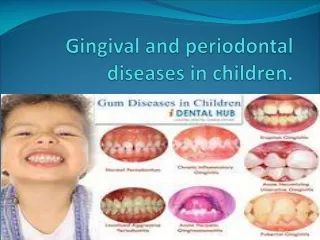
Gingival and periodontal diseases in children. The gingiva forms the important part of the periodontium,the supporting structure of the tooth. Gingiva is a masticatory type of oral mucous membrane,forms the covering of the teeth. 3parts:- Marginal gingiva. Attached gingiva.

E N D
The gingiva forms the important part of the periodontium,the supporting structure of the tooth.
Gingiva is a masticatory type of oral mucous membrane,forms the covering of the teeth. • 3parts:- • Marginal gingiva. • Attached gingiva. • Interdental gingiva
Marginal Gingiva:- • Gingival crevice or the sulcus and a free gingival margin. • Free gingival margin-thicker and rounded-primary teeth due to morphological characterstics-cervical bulge and underlying constriction at CEJ. • Knife edge in permanent dentition.
Marginal gingiva-flaccid and retractable Immature connective tissue . Immature gingival fiber system. Increased vascularisation.
Attached gingiva:-continuous with the marginal gingiva.It is firm and resilient and tightly bound to the underlying periosteum of alveolar bone.(adult) • Less dense and more redder in children-less keratinised and more vascular supply. • More flaccid-lesser connective tissue density. • Less stippled.
Interdental clefts and retrocuspid papilla. • Interdental clefts-interradicular zones underlying the saddle areas. • Retrocuspid papilla-1mm below the free gingival groove on attached gingiva lingual to mandibular canine.-dec .with age.
Interdental gingiva:-interdental spacing. Saddle areas-well keratinised.less risk of development of inflammatory lesions. Low prevalance of periodontal lesions in children.
Alveolar mucosa:-thin epithelium absence of keratin-redder than pink. More elastic fibers-moveable. Width increases with age and tooth eruption.
Gingival sulcus:-shallow crevice or space around the tooth bounded by the surface of tooth on one side and the epithelium lining the free margin of the gingiva on the other. normal depth is 2-3mm. Primary dentition it more mean value range from 1.4mm-2.1mm
Alveolar bone:-less calcified,more vascular,larger marrow space,thin lamina dura,flat interdental crests.
Why only gingivitis Less periodontitis in children- • A)More anabolic activity due to increase metabolism. • B)Absence of bacteria responsible for periodontal disease-Spirochetes and B.melaninogenicus. • C)Altered composition of plaque. • D)Decreased leukocytic migratory rate –low levels of immmunoglobulins specific for plaque bacteria.
Physiologic changes associated with tooth eruption:- Pre-eruptive stage. Eruptive stage. Post eruptive stage.
Gingivitis:-inflammatory involvement of gingival tissues. Inflammatory exudate Edema. Destruction of collagenous gingival fiber. Ulceration of epithelium.
Stages of gingivitis:- Stage1:-Initial lesion 2-4days Mild change in color. Vascular dilatation. Junctional epithilium and sulcular epithelium-infiltrated by polymorphonuclear cells.
Stage 2:- 4-7days. More vascular proliferation. Junctional and sulcular epithelium-infiltrated by polymorphonuclear cells,rete pegs formation. Lymphocytes are predominent. Loss of collagen. c/f-erythema,bleeding on probing
Stage3:-Established lesion 14-21 days. Increased vascular proliferation and blood stasis. More severe changes seen in junctional and sulcular epithelium. Severe loss of collagen. Plasma cells are predominent. Changes in color,size,texture
Stage 4:-advanced lesion. Lesion extends in to alveolar bone. Periodontal distruction. Clinical features:- Gingival bleeding. Change in color. Change in the consistency of gingiva. Changes in the surface texture of the gingiva.
Etiology of gingival diseases:- 1.Local irritating factors:- A)bact.plaque. B)predisposing factors:- material alba,food debries,malalignment of teeth,dental calculus.
2)Local functioning factors:- • A)Malocclusion • B)Habits • 3)systemic factors:- • A)Puberty. • B)Vitamin or protein deficiency. • C)Drugs and chemicals. • D)Pregnancy.
E)Metabolic disorder. D)Viral,bacterial and fungal infection.
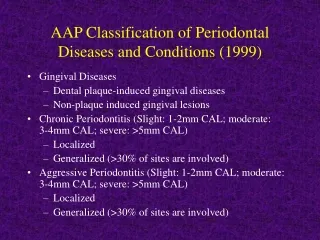
Classification of gingival diseases:- A)Simple gingivitis. 1)Eruption gingivitis. 2)Gingivitis associated with poor oral hygiene. B)Acute gingival inflammation. 1)Herpes simplex virus infection. 2)Recurrent apthous ulcer.
3)Acute necrotizing ulcerative gingivitis. 4)Acute candidiasis. 5)Acute bacterial infection. C)Chronic non specific gingivitis.
D)Conditioned gingival enlargement. • 1)Puberty gingivitis. • 2)Fibromatosis. • 3)Phenytoin-induced gingival overgrowth. • E)Scorbutic gingivitis
simple gingivitis:- a)Eruption gingivitis:- Treatment:-pericoronitis-phenol 5%,15ml of tincture of iodine and 20ml of glycerine. Pericoronitis with swelling and lymphnode enlargement.antibiotics
b)Gingivitis associated with poor oral hygiene.or chronic marginal gingivities: Etiology: plaque. Marginal and papillary gingiva. Localised or generalised . Treatment: oral prophylaxis
Gingival abscess:- Localised painful,rapidly expanding lesion-sudden onset. Marginal gingiva or interdental gingiva. Initially appears as a red swelling with smooth shiny surface. 24-48hrs it becomes fluctuant and pointed.-purulent exudate. Adjacent teeth –sensitive
Etiology. Impacted foreign substance. Treatment:- Topical LA-incision-drain the pus-cleansed with saline or warm water-gauze pad. Home-warm water rinse.
Viral:- • Acute herpetic gingivostomatitis • 2 types of HSV. • HSV-1-upper part of body. • HSV-2.-lower part of the body.
Rarely occur before the age of 6 months presence of circulating antibodies.in the infants ,derived from the mother. Focal itching ,burning or tingling sensations on the lips -1-7 days. This may be proceeded by stress,strain,oral trauma,pharyngitis,sinusities .
Condition occurs during and immediately after an episode of pneumonia, typhoid and influenza • Development of fever ,irritability, head ache, pain upon swallowing and regional lymphadenopathy.
Diffuse, erythematous ,shiny involvement of the gingiva and adjacent oral mucosa . With in a few days the mouth becomes painful and gingiva intensely inflamed. Lips ,tongue,buccalmucosa,palate,tonsil shows swelling
Shortly a yellowish ,fluid filled vesicles develop. These rupture and to form shallow,ragged,extremely painful ulcers covered by a grey membrane and surrouned by an erythematous halo.
“Soreness” of the oral cavity. Difficulty in mastication. They heal spontaneously with in 7-14 days and leave no scar. Differential diagnosis:-Acute necrotizing ulcerative gingivities. Canker sore,Erythema multiforme.
Treatment:- Application of mild topical anaesthetic – Dicyclomine HCL(0.5%) before mealtime . Lidocaine -topical LA.-tell them to hold it in mouth for 2-3 minutes. Vitamin supplement. Acyclovir.(Zovirax)
Acute necrotising ulcerative gingivities: Trenchmouth,vincent’s angina or stomatitis. Etiology:-Fusiform bacilli, spirocheates. Local factors-over hangingrestoration,malocclusion. Systemic factors-stress. Nutritional deficiency-VitaminB ,VitaminC. Debilitating diseasesDown’syndrome,AIDS,diabetes
C/f:- Primary diagnostic signs:-gingival bleeding . Interdental ulceration and necrosis. Blunting and cratering of gingiva. Elevated temperature.
Secondary diagnostic feature. Pseudomembrane. Fetid odor. Bad taste-mandibular anteriors. Wooden sensation of teeth.
Severe cases systemic complications-high fever,lymphadenopathy,increased pulse rate,anorexia. Treatment:- Local debridement ,sub gingival curettage . Mild oxygenating solutions.
Penicillins/erythromycin,metranidazole. NSAIDS. Fluid consumption. Bed rest.
Drug induced gingival hyperplasia:- Phenytoin,cyclosporine,nifedipine. c/f:- 2-3weeks after initiation of phenytoin therapy. Painless enlargement of interproximal gingiva. Buccal and ant.segment more than lingual and posterior.
Gingiva -pink and firm unless infected. No bleeding . Interdental lobulations-clefting-pseudopockets. Difficulty in mastication,speech. Treatment:- maintenance of oral hygiene. Change of drug or drug dossage. Surgical excision.