Download
1 / 26
410 likes | 1.23k Views
Ventilation/Perfusion Relationships Dr.Shafali Singh. Learning objectives. Identify the average V/Q ratio in a normal lung. Explain how V/Q is affected by the vertical distribution of ventilation and perfusion in the healthy lung.

E N D
Learning objectives • Identify the average V/Q ratio in a normal lung. Explain how V/Q is affected by the vertical distribution of ventilation and perfusion in the healthy lung. • Describe how the ventilation/perfusion (V/Q) ratio of an alveolar-capillary lung unit determines the PO2 and PCO2 of the blood emerging from that lung unit. • Describe the normal relative differences from the apex to the base of the lung in alveolar and arterial PO2, PCO2, pH, and oxygen and carbon dioxide exchange. • Describe causes of abnormal V/Q distribution and predict how the presence of abnormally low and high V/Q ratios in a person's lungs will affect arterial PO2 and PCO2. • Define right-to-left shunts, anatomic and physiological shunts, and physiologic dead space (wasted ventilation).
PERFUSION(Q) • Perfusion is the process by which deoxygenated blood passes through the lung and becomes reoxygenated. • The arteries of the pulmonary circulation are thin walled, with minimal smooth muscle. • Vessels are very compliant, low-resistance circulatory system
Q. Which of the following best characterizes the pulmonary circulation? Flow Pressure Resistance Compliance (A) Low High Low High (B) High Low High Low (C) Low LowLow High (D) High Low High High (E) High Low Low High
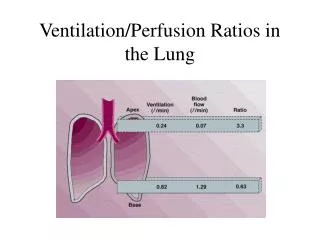
Distribution of Pulmonary Blood Flow The distribution of pulmonary blood flow within the lung is uneven and the distribution can be explained by the effects of gravity. When a person is supine, blood flow is nearly uniform, since the entire lung is at the same gravitational level. However, when a person is upright, gravitational effects are not uniform, and blood flow is lowest at the apex of the lung and highest at the base of the lung. Each lung is divided into three zones in upright position based on the effect of gravity.
Question The effect of gravity on the pulmonary circulation in an upright individual will cause (A) Blood flow to be the greatest in the middle of the lung (B) Capillary pressure to be greater at the base of the lung compared with the apex (C) Alveolar pressure to be greater than capillary pressure at the base of the lung (D) Lower vascular resistance at the apex of the lung compared with the base (E) Venous pressure to be greater than alveolar pressure at the apex
Question Lowering pulmonary venous pressure will have the greatest effect on regional blood flow in (A) Zone 1 (B) Zone 2 (C) Zone 3 (D) Zones 1 and 2 (E) Zones 2 and 3
Ventilation/perfusion ratios Q = 5,000ml/min
Ventilation/perfusion ratios The ventilation/perfusion ratio (V/Q) is the ratio of alveolar ventilation (VA) to pulmonary blood flow (Q). Matching ventilation to perfusion is critically important for ideal gas exchange. The normal value for V/Q is 0.8. This value means that alveolar ventilation (L/min) is 80% of the value for pulmonary blood flow (L/min).
Question Which of the following best characterizes alveolar ventilation and blood flow at the base, compared with the apex, of the lungs of a healthy standing person? Ventilation Blood flow Ventilation perfusion ratio (A) Higher Higher Lower (B) Lower Higher Higher (C) Lower LowerLower (D) Higher Lower Higher (E) Lower Lower Higher
VA/Q= INFINITY • When perfusion is 0, VA/Q = infinity & constitutes DEAD SPACE • The alveolar air becomes equal to the humidified inspired air. That is, the air that is inspired loses no oxygen to the blood and gains no carbon dioxide from the blood. • And because normal inspired and humidified air has a PO2 of 150 mm Hg and a PCO2 of 0 mm Hg, these will be the partial pressures of these two gases in the alveoli
VA/Q =0 • When ventilation is 0, VA/Q =0 & constitutes PHYSIOLOGICAL SHUNT • that is, without any alveolar ventilation—the air in the alveolus comes to equilibrium with the blood oxygen and carbon dioxide because these gases diffuse between the blood and the alveolar air. • This causes 1) LOW arterial PO2 because of admixture of venous blood with arterial blood 2)Alveolar PO2 is less than 100 mm Hg
Effect of regional differences in ventilation/perfusion (V/Q) on PCO2 and PO2
Question Regional differences in ventilation perfusion ratios affect gas tensions in the pulmonary blood. Which of the following best describes the gas tensions in the blood leaving the alveolar capillaries of a healthy standing individual? O2 tension (PO2) CO2 tension (PCO2) (A) Lowest at base Highest at apex (B) Highest at base Lowest at base (C) Highest at apex Lowest at apex (D) Highest at apex Lowest at base (E) Lowest at base Lowest at base
Question Patient A is having V/Q ratio : 0.49 Patient B is having V/Q ratio : 0.41 Which among these two will have? • Higher pO2 • Higher pCO2 • High pH