Download
1 / 46
460 likes | 585 Views
Endocrine Conference. 2004. 6. 22 Department of Surgery R2. Heung Kwon Oh M.D. Case 1. 박 O O F/49 C.C) Thyroid nodule detected by routine check P.I) #1. Known HBsAg carrier

E N D
Endocrine Conference 2004. 6. 22 Department of Surgery R2. Heung Kwon Oh M.D.
Case 1 박O O F/49 C.C) Thyroid nodule detected by routine check P.I) #1. Known HBsAg carrier #2. 2004년 1월 인근병원에서 시행한 건강검진 상 좌측 갑상선 결절 발견되어 Fine needle aspiration cytology 검사결과 thyroid cancer진단 하에 수술 위해 의뢰되어 본원외과 외래 통해 입원함
#3. Outside neck sono (2004.1.19) 4.4x5.7x5.9mm sized ill defined hypoechoic nodule in Lt thyroid gland -> r/o malignancy #4. Outside FNAC (2004.2.5) smear and cell block reveal a few papillary clusters of typical follicle cells having frequent nuclear grooves and inclusion -> compatible with PTC
PMHx) DM/HT/Tbc/Liver Ds ( - / - / - / + ) Op Hx ( - ) Allergic Ds ( - ) Neck irradiation Hx ( - ) FHx) No Hx of thyroid ds. S/R) E/F ( - ), G/W ( - ), Wt loss ( - ) A/N/V/D/C ( - / - / - / - / - ), H/M/H ( - / - / - ) chest pain/palpitation/dyspnea ( - / - / - ) voice change ( - ), C/S/R ( - / - / -) Urinary Sx ( - )
Physical Examination V/S 121/64 – 76 – 18-36.9 G/A not so ill-looking, alert and intact HEENT not anemic, anicteric not dehydrated tongue PI ( - ), PTH ( - / - ) Neck no definite palpable mass LNE ( - / - ) Chest CBS without rale RHB without murmur Abdomen soft, flat no palpable mass normoactive BS , T/RT ( - / - ) Back and Ext. CVAT(-/-), P/C/C(-/-/-)
Laboratory study TFT) T3 96 (87 ~184) fT4 0.90 (0.7~1.8) TSH 0.22 (0.4~4.1) Tg 17.2 (0 ~52) Tg-Ab 38 (0 ~100) Routine lab) WNL
Neck CT(2004.3.16) 1) A small nodule at Lt thyroid gland posterior aspect. 2) No significant nodal enlargement
2004.3.26 Total thyroidectomy Op finding) Lt lobe 0.6cm sized, solid, poorly encapsulated mass Capsular invasion ( + ), Adjacent structure invasion ( - ), Lt lobectomy -> frozen ; PTC -> total thyroidectomy LNE ( - ) Parathyroid gl. & recurrent laryngeal n. : saved
Hospital course 2004.3.29 Discharge without immediate postop complication
Pathology Thyroid, bilateral, total thyroidectomy: 1. Papillary microcarcinoma, left lobe with 1) size: 0.3 x 0.3 x 0.2cm 2) confinement to thyroid 3) clear resection margin 2. Adenomatous goiter, right lobe
Case 2 최 O O (F/26) C.C) Neck mass(onset : 3MA) P I) #1. Prev. healthy #2. 3MA 우연히 Rt neck mass (not tender, firm) 발견하여 인근병원 방문후 큰병원 권유받고 r/o thyroid cancer로 FNAC 시행후 highly suggestive PTC소견보여 수술 권유받았으나 환자, 보호자 원하여 본원 외과 외래 방문 후 수술 위해 입원함.
PMHx) DM/HT/Tbc/Liver Ds ( - / - / - / - ) op Hx ( - ) Allergic ds (-) Neck irradiation Hx ( - ) FHx) No Hx of thyroid ds. S/R) E/F ( - ), G/W ( - ), Wt loss ( - ) A/N/V/D/C ( - / - / - / - / - ), H/M/H ( - / - / - ) chest pain/palpitation/dyspnea ( - / - / - ) voice change ( - ), C/S/R ( - / - / -) Urinary Sx ( - )
Physical Examination V/S 110/70 – 70 – 20 – 36.5 G/A Not so ill-looking, alert and intact HEENT not anemic, anicteric PI(-), PTH(-/-) Neck 3x2cm sized, firm, fixed, ill - defined mass in Rt thyroid gland LNE ( + / - ) level lll 1cm firm Chest CBS without rale RHB without murmur Abdomen Soft, flat normoactive BS T/RT(-/-) Back and Ext. CVAT(-/-), P/C/C(-/-/-)
Laboratory Study TFT) T3 112 (87 ~184) fT4 1.27 (0.7~1.8) TSH 3.01 (0.4~4.1) Tg 61.4 (0 ~52) Tg-Ab 491 (0 ~100) Routine lab) WNL
Neck CT(2004.3.16) 1) 2cm sized nodule at Rt thyroid gland 2) LNE in right level III, submental space
2004.4.6 Total Thyroidectomy, Rt MRND Op finding) Rt lobe 3x4cm sized, solid, poor encapsulated mass Capsular invasion ( + ), Adjacent structure invasion ( - ), Rt lobectomy -> frozen; PTC -> Total thyroidectomy multiple Rt cervical LNE ( + ) -> Rt MRND Parathyroid gl. & recurrent laryngeal n. : saved
Hospital course 2004.4.9 Discharge without immediate postop complication
Pathology Thyroid, bilateral, total thyroidectomy, Rt MRND: 1. Papillary carcinomas (x2), right lobe 1) tumor size; 1.5 x 1.5 x 1cm and 2 x 1 x 1cm 2) confinement to thyroid parenchyme 3) no endolymphatic tumor emboli 4) clear soft tissue resection margin 5) metastasis in four out of eight regional lymph nodes 2. Chronic lymphocytic thyroiditis, left lobe
Papillary thyroid cancer Randolph et al ; Surgery of the thyroid and parathyroid glands - chapter 15, papillary carcinoma of the thyroid
Thyroid Neoplasm Solitary nodule in the thyroid gland prevalence : increased with age averaging 6.4% of women, 1.5% of men autopsy study : as many as 50 % of necropsies Overall incidence of malignancy : 20% ~ 30% in surgical series
Evaluation of Patients with thyroid nodules History taking 1) Radiation 2) Time of onset 3) Age and sex 4) Preexisting thyroid disease 5) Voice change, dysphagia, dyspnea 6) Pharmaceutical agents and toxins lithium, phenobarbital : TSH↑ 7) Familial Hx : MTC, Gardner’s syn. Cowden’s disease
Evaluation of Patients with thyroid nodules Physical Examination solitary or multinodular hard, firm, ill-defined margin hoarsness, unilateral vocal cord paralysis cervical adenopathy
Evaluation of Patients with thyroid nodules Diagnostic tests 1. Fine-needle aspiration biopsy malignant intermediate ; 10 ~ 30 % cancer benign
Evluation of Patients with thyroid nodules 2.Ultrasound noninvasive, inexpensive, objectively follow the size 3.Thyroid scan cold nodule vs hot nodule 4.Chest radiograph 5.CT and MRI useful in evaluating with suspected aggressive carcinomas
Benign Family Hx of benign goiter Diffuse or multinodular goiter Constant size Benign by FNA Simple cyst by USG Hyperfuctioning nodule by radioiodine scan Decreasing size with thyroid hormone replacement Malignant Solitary nodule Hard, fixed Rapidly enlarging Hoarseness with vocal cord paralysis Development of nodule at age <25 or >60 years Suspicious or malignant by FNA Cyst > 4cm or complex cyst Hypofuctioning by scan Hx of ionizing radiation Ipsilateral lymphadenopathy Characteristics of Benign and Malignant Thyroid Nodules
Thyroid cancer Well differentiated cancer in the USA Papillary carcinoma 79.25% Follicular carcinoma 12.55% Hurthle cell carcinoma 2.94% Poorly differentiated cancer Medullary carcinoma 3.57% Anaplastic cancer 1.65% Lymphoma Sarcoma Metastastic cancer (Hundahl SA et al : Cancer 83:2638, 1988)
Papillary thyroid cancer • Pathologic feature • Predisposing factor • Typical presentation • Diagnosis • Extent of initial surgery • Risk factor evaluation for prognosis • Adjuvant therapy • Follow up
Introduction • Follicular cell-derived W/D cancer • After treatment, cure or die from other causes • 85 % of thyroid ca • Children and young women (mean age 44) • Prior exposure to ionizing radiation Hx • Familial PTC (5~10%) • Gene rearragement; ret/PTC, NTRK1
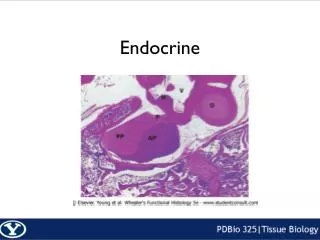
Pathologic feature • A malignant epithelial tumor showing follicular cell differentiation and the formation of papillae and/or nuclear changes • Orphan Annie eye; empty nucleaoplasm • Psammoma body • Papillary thyroid microcarcinoma (PMC) • Multicentric involvement (30%) • Extrathyroidal involvement (14%) • Metastasis to cervical LN (35%)
Pathologic feature FNA from normal thyroid: sheets of follicular cells with uniform round evenly spaced nuclei and some macrofollicles filled with colloid. FNA from PTC: sheets of follicular cells with overlapping and crowded oval nuclei which show longitudinal nuclear grooves. .
Diagnosis • Hx and P/E • Thyroid function test • Thyroglobulin (Tg) • Radioisotope scan; little useful • USG (Power doppler tech); nodule • CT, MRI; invasion • FNA; primary test • PCR; oncofetal fibronectin mRNA
Extent of surgery • Complete resection of primary tumor and any locoregional extension is essential • Bilateral lobar resection > lobectomy • Local recurrence, survival rate • Adjuvant therapy, postop f/u • Multicentricity, anaplastic transformation • Total thyroidectomy = Near total thyroidectomy • Complication rate • But experienced surgeon • Central LND ± MRND ?
Poor prognostic factors • Incomplete resection • Extrathyroidal invasion • Intrathyroidal microvascular invasion • Male sex, old age ( > 50 yr) • Tumor size • Distant metastasis at presentation • LN meta, local recurrence ; no impact
TNM staging (AJCC) T ; primary tumor T0 No evidence of primary tumor T1 Tumor ≤ 1cm T2 1cm < Tumor < 4cm T3 Tumor > 4cm T4 Tumor of any size extending beyond the thyroid capsule N ; regional LN N0 ( - ) regional LN metastasis / N1 (+) M ; distant metastasis M0 ( - ) distant metastasis / M1 ( + )
AMES catergory ; 박 O O F/49 Thyroid, bilateral, total thyroidectomy: 1. Papillary microcarcinoma, left lobe with 1) size: 0.3 x 0.3 x 0.2cm 2) confinement to thyroid 3) clear resection margin 2. Adenomatous goiter, right lobe Low risk patient
AMES catergory ; 최 O O F/29 Thyroid, bilateral, total thyroidectomy, Rt MRND: 1. Papillary carcinomas (x2), right lobe 1) tumor size; 1.5 x 1.5 x 1cm and 2 x 1 x 1cm 2) confinement to thyroid parenchyme 3) no endolymphatic tumor emboli 4) clear soft tissue resection margin 5) metastasis in four out of eight regional lymph nodes 2. Chronic lymphocytic thyroiditis, left lobe Low risk patient
Adjuvant therapy • Thyroxine therapy • 2.2 ~ 2.8 μg / kg / day • TSH suppression -> significant reduction in progression -> TSH < 0.1 (high risk group) -> 0.1 < TSH < 0.4 (low risk group) • Radioiodine remnant ablation • Local or distant residual disease (+) • More selective approach is needed
Follow-up and risk group • Tg ; useful tumor marker • TgAb, TSH • USG • Chest PA • CT, Bone scan • Radioiodine whole body scan • TSH defendent • PET