Download
1 / 65
910 likes | 2.4k Views
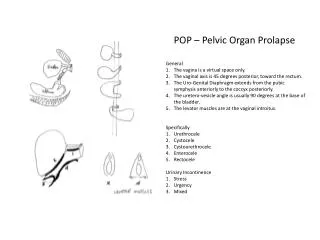
Pelvic organ prolapse. POP. Rectocele. Rectocele. COCHRIAN REWIEW 50 % of women with history of delivery have pelvic organ prolapse. RECTOCELE ASSOCIATED WITH : SI. 30% Rectal prolapse. 33% Anismus . 10% Enterocele 2%.

E N D
COCHRIAN REWIEW 50% of women with history of delivery have pelvic organ prolapse
RECTOCELE ASSOCIATED WITH: • SI. 30% • Rectal prolapse. 33% • Anismus. 10% • Enterocele2%
42% of gynecologist's elective operations are RECTOCE • BUT • 16% of these patients are evaluated correctly • 85% of patients who are candidate for surgery by • proctologists ,have systematic evaluations
Bowel Bladder Sexual The effect of pop surgery on Function UNPREDICTABLE
Definition of cure in surgical treatment • No anatomic prolapse • No functional symptoms • Patient satisfaction • Avoidance of complication
In upper vaginal vault prolapse which option is preferred? -Abdominal approach(sacrocolpopexy) -Vaginal approach(sacrospinousfixation&post.colporraphy)
Uterine or vaginal vault prolapse Abdominal sacrocolpopexy is better than vaginal sacrospinousfixation
In abdominal approach: -laparascopic -open. hysterectomy or Levatormyorraphy With&without
Comprehension of abdominal sacrocolpopexy&vaginalsacrospinousfixation: Abdominal approach has lower recurrence Less Dysparunia Longer operating time Longer recovery time Higher cost
In post.vaginal wall prolapse which approach has low recurrence ? Post.colporraphy with or without graft Transanal repair √Abdominal post.repair
In rectocele, vaginal approach is superior to transanal approach.
In post.colporraphy: -traditional colporraphy -mesh
Use of graft: Yes or No?
What kind of graft? -synthetic -Biologic. (autologous,alloplastic,cadave)
Use of absorbable or nonabsorbable graft in cystocele repair: Reduce the risk of recurrent cystocele on examination The effect of graft in patient's satisfaction & QOL is uncertain
In continent women, concomitant continence surgery don't reduce the rate of post.op SI In occult SI, concomitant continence surgery : 20% prevent of post op SI 60% will have unnecessary procedure For balance between cost&side effect more investigation must be done
Rectocele&ant,compartment prolapse: -Traditional ant.repair -Burch operation -Mesh
What kind of suture? -Absorbable -Non absorbable
Small enterocele : transperineal Large enterocele: transabdominal
Transperineal. If there is gap in Endoanalsono:+ Sphincteroplasty If there is no gap: + Levatoroplasty
Rectocele&(no anismus , no anorectal problem , no severe dyspaurunia , no fecal incontinence): Transvaginal & site specific repair
Comprehension of surgical repair with conservative management of pop: There is no any research .
Comprehension of surgical repair with mechanical device There is no any research .
Figure 1. Commonly used pessaries: (A) Smith; (B) Hodge; (C) Hodge with support; (D) Gehrung; (E) Risser; (F) Ring with diaphragm; (G) Ring; (H) Cube; (I) Shaatz; (J) Rigid Gellhorn; (K) Flexible Gellhorn; (L) Incontinence ring; (M) Inflatoball; (N) Donut. Image courtesy of CooperSurgical, Inc., Trumbull, CT.
Indication of STARR : Rectocele with&withoutIRP