Download
1 / 25
260 likes | 521 Views
NUR 142: skill 35-1. POUCHING A COLOSTOMY OR AN ILEOSTOMY. OSTOMY CARE – INTRODUCTION: Certain diseases or conditions require surgical intervention to create an opening into the abdominal wall for fecal or urinary elimination.

E N D
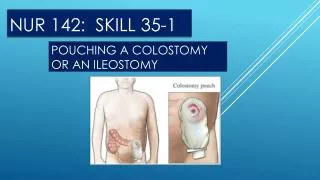
NUR 142: skill 35-1 POUCHING A COLOSTOMY OR AN ILEOSTOMY
OSTOMY CARE – INTRODUCTION: • Certain diseases or conditions require surgical intervention to create an opening into the abdominal wall for fecal or urinary elimination. • Examples of these conditions include cancer, inflammatory bowel disease, perforation of the colon, or fecal incontinence. • The opening is called a stoma and it is constructed from a section of colon or small intestine. • The output from the stoma is called the effluent. • An opening in the large intestine or colon is a colostomy.
OSTOMY CARE – CONT’D • A colostomy in the descending or sigmoid colon generally results in a stool similar to that normally passed through the rectum. • If the opening is in the transverse or ascending colon, the effluent varies from thick liquid to semi-formed stool. • An opening in the ileal portion of the small intestine is an ileostomy, and the fecal effluent will be watery-to-thick liquid and contain some digestive enzymes. • Fecal ostomies are either temporary or permanent, depending on the underlying condition and the surgical procedure performed.
OSTOMY CARE – CONT’D • A urostomy or ileal conduit is created from a portion of the intestine that is resected from the ileum. • One end of the conduit is sutured closed, and the ureters are implanted through mucosa. • The other end is brought out on the abdominal wall, and a stoma is formed for urine to exit the body. This ostomy is permanent. A patient with a colostomy, ileostomy, or ileal conduit has not sensation or control over the time or frequency of the output and must wear a pouch to collect the effluent.
OSTOMY CARE – CONT’D • Surgical procedures to create continent internal fecal or urinary pouches eliminate the need for an eternal pouch. • The continent ileostomy is a pouch made from a segment of the ileum and placed under the abdominal wall, with a small tract from the pouch opening through the skin. • A patient inserts a large catheter through this opening or stoma several times a day to empty fecal effluent in the internal pouch. • These procedures are done less frequently now because there are other surgical options available with higher long-term success rates.
OSTOMY CARE – CONT’D • There are two types of continent urinary diversions. • One is a continent urinary reservoir created from the intestine. • This reservoir into which the ureters are inserted is situated under the abdominal wall, with a narrow tract coming out through the abdominal wall to form a small stoma. • A catheter is inserted to empty the urine from the pouch. • Patients must be able and willing to catheterize the pouch 4 to 6 times a day for the rest of their lives. • The other type of continent urinary diversion is an orthopic neo-bladder, which also uses an intestinal pouch to replace the bladder
PRIMARY CHANGES IN OSTOMY CARE: • One of the primary changes in ostomy care is related to stoma care. • Pouching systems are more effective, and adhesive technology are more advanced. • Remember, this is all new to the patient and it is important to help them adjust to this! • This doesn’t change who a person is at heart!
These improvements include a wider variety of sizes and shapes of the skin barriers, depths of convexity from shallow to deep, and degree of flexibility: • The current trend is to apply a pouch directly to clean, dry skin without using skin preparations, paste, or added adhesives unless a patient has a specific problem keeping a pouch intact. • The adhesives on the skin barriers are pressure and heat sensitive; thus a patient should apply gentle pressure with the hand over the skin barrier for several minutes to adhere the barrier to the skin. • There are new and improved accessory products such as rings or seals for managing abdominal contours that are uneven or peri-stomalskin that is not intact
PRIMARY CHANGES IN OSTOMY CARE – CONT’D • Some pouches have effective gas filters that allow flatus to escape slowly from the pouch through a charcoal filter. This filter absorbs odor and does not allow leakage of liquid effluent through the filter. • All of the ostomy companies now have pouches with integrated closures. A Velcro-like closure eliminates the need for a clip to close the bottom of the pouch. It also requires less manual dexterity to empty the pouch. • A wider selection of products for neonatal and pediatric use has improved the care of the population.
PATIENT CENTERED CARE: • With any ostomy requiring a pouching system, a secure seal to prevent leakage of the effluent and protect the skin around the stoma (peristomal skin) is vital to helping patients resume normal activities and accept the changes in their bodies as a result of surgery. • It is also a very important factor in facilitating the emotional adjustment to the ostomy. • In addition to the stress of illness and surgical recovery, patients with ostomies face body image changes, fear of social rejection, concern about sexual function and intimacy, and the need for help with personal care. • As you communicate with a patient during ostomy care, be sensitive and avoid communicating anything that the patient may interpret as disrespect or disgust. • A supportive nurse makes the initial period of adjustment easier.
SAFETY GUIDELINES: • 1. Change ostomy pouches before they become full to avoid leakage, which can lead to chemical or enzymatic injury to the skin. • 2. Wear gloves during pouch and stoma care to reduce exposure and transmission of infectious microorganisms. • 3. Know the signs of a healthy stoma and peri-stomal skin: • Color/moisture: Stoma should be red or pink and moist. Report a gray, purple, or black stoma to the charge nurse or health care provider. • Size: In the 4 to 6 weeks after surgery, the stoma will likely decrease in size. Measure with each pouch change. • Peristomal skin normally is intact with some reddening. Presence of blisters, a rash, or raw-like appearance is abnormal.
SKILL 35-1: POUCHING A COLOSTOMY OR AN ILEOSTOMEY – LET’S BEGIN! • Immediately after a fecal surgical diversion, it is necessary to place a pouch over the newly created stoma to contain effluent when the stoma begins to function. • The pouch will keep a patient clean and dry, protect the skin from drainage, and provide a barrier against odor. • A cut-to-fit, transparent pouching system is preferred because it will cover the peri-stomal skin without constricting the stoma and allow for visibility of the stoma.
ASSESSMENT: • 1. Perform hand hygiene and apply clean gloves. • 2. Observe existing skin barrier and pouch for leakage and length of time in place. Pouch should be changed every 3 to 7 days for colostomy and 3 to 5 for ileostomy, no daily. In case of an opaque pouch, remove it to fully observe the stoma. • 3. Observe the amount of effluent in the pouch and empty it if it is more than one-third full by opening clip and draining it into a container for measurement of output. Note consistency of effluent and record intake and output. • 4. Observe stoma for type, location, color, swelling, presence of sutures, trauma, and healing or irritation of peri-stomal skin. Remove and dispose of gloves.
ASSESSMENT - CONT’D • 5. Observe abdomen for best type of pouching system. Consider: • A. Abdominal contour • B. Presence of scars or incisions. • Abdominal contours, scars, or incisions affect type of system and adhesion to skin surface. • 6. Explore patient’s attitude toward learning self-care and identify others who will be helping patient after leaving hospital.
PLANNING: • 1. Expected outcomes following completion of the procedure: • Stoma is moist and reddish pink. Skin is intact and free of irritation; sutures are intact. • Stoma drains moderate amount of liquid or soft stool, and flatus is in pouch (noted by bulging of the pouch). (Flatus may not be observable if pouch has gas filter). • Patient, family caregiver, and/or significant others observe stoma and steps of procedure. • Patient asks questions about procedure and attempts to help with pouch change.
PLANNING – CONT’D • 2. Explain procedure to patient; encourage patient’s interaction and questions. • 3. Assemble equipment and close room curtains or door – optimizes use of time; provides privacy.
IMPLEMENTATION • 1. Identify patient using two identifiers. • 2. Position patient in semi-reclining or supine during assessment and pouching (Note: Some patients with established ostomies prefer to stand). If possible, provide patient with mirror for observation. • 3. Perform hand hygiene and apply clean gloves. • 4. Place towel or disposable waterproof barrier under patient and across patient’s lower abdomen.
IMPLEMENTATION – CONT’D • 5. If not done during assessment, remove used pouch and skin barrier gently by pushing skin away from the barrier. Use an adhesive remover to facilitate removal of skin barrier. Empty pouch and dispose of it in an appropriate receptacle. Measure output, if needed. • 6. Clean peri-stomal skin gently with warm tap water using wash cloth; do not scrub the skin. If you touch the stoma, minor bleeding is normal. Pat the skin dry. When pouching an ileostomy, place disposable wash cloth over the stoma.
IMPLEMENTATION – CONT’D • 7. Measure the stoma. Expect size of stoma to change for the first 4 to 6 weeks after the surgery. • 8. Trace pattern of stoma measurement on pouch backing or skin barrier. • 9. Cut opening on backing or skin barrier wafer. Be sure that opening is at least 1/8 larger than the stoma to avoid pressure on it.
IMPLEMENTATION – CONT’D • 10. Remove protective backing from adhesive. • 11. Apply pouch over stoma. Press firmly into place around stoma and outside edges. Have the patient hold hand over the pouch to apply heat to secure the seal. • 12. Close the end of the pouch with a clip or integrated closure. Remove the drape from the patient. • This ensure that the pouch is secure. Contains Effluent • 13. Remove gloves. Perform hand hygiene.
EVALUATION: • 1. Observe condition of the skin barrier and adherence to abdominal surface • Determines the presence of leaks • 2. Observe appearance of stoma, peri-stomal skin, abdominal contours, and suture line during pouch change. • Provides information if another type of pouching system or additional skin care products are needed. • 3. Observe patient’s and family caregiver’s willingness to view stoma and ask questions about the procedure. • Determines level of adjustment and understanding of stoma care and pouch application. • Allows planning for future education needs and progress toward acceptance of altered body image.
UNEXPECTED OUTCOMES: • 1. Skin around the stoma is irritated, blistered, or bleeding, or a rash is noted. May be caused by un-determining of pouch seal by fecal contents, allergic reaction, or fungal skin eruption. • 2. Necrotic stoma is manifested by purple or black color, dry-instead of-moist texture, failure to bleed when washed gently, or tissue sloughing. • 3. Patient refuses to view stoma or participate in care.
RECORDING AND REPORTING: • 1. Record type of pouch and skin barrier applied, amount and appearance of effluent in pouch, size and appearance of stoma, and condition of peri-stomal skin. • 2. Record patient/family level of participation, teaching that was done, and response to teaching. • 3. Report any of the following to nurse and/or health care provider: Abnormal appearance of stoma, suture line, peri-stomal skin, or character of output.
THIS IS THE END OF THE SKILL • Your book has provided a video for this skill, which is, as follows: • http://bookstie.Elsevier.com/Perry-Potter/ClilnicalSkills/video42.php • Elsevier: Perry-Potter: Clinical Nursing Skills and Techniques. 8e-35.1. Pouching a colostomy or Ileostomy.