Download

1 / 13
820 likes | 2.56k Views
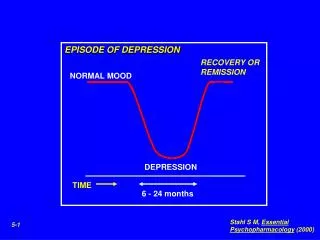
Depression. Objectives. Background. Prevalence rates for depression: 1% to 2% of prepubertal children 3% to 8% of adolescents. Depression and bipolar disorder equally common in both sexes. Unipolar depressive disorders in teens more common in girls than in boys (ratio of 3:1)

E N D
Background • Prevalence rates for depression: • 1% to 2% of prepubertal children • 3% to 8% of adolescents. • Depression and bipolar disorder equally common in both sexes. • Unipolar depressive disorders in teens more common in girls than in boys (ratio of 3:1) • Early onset of puberty in girls increases the risk for depression.
Clinical Features & When to Consider Diagnosis • Sad, irritable, or angry • may present with school or behavioral problems • Somatic complaints • headache, stomachache, muscle weakness, decreased or increased appetite, fatigue, insomnia, hypersomnia, or disturbed sleep-wake cycles • Self-injurious behaviors or suicidal ideation, plan, and intent
Identifying Risk FactorsEnvironmental • Abuse or neglect • Parental substance abuse • Marital problems • Low socioeconomic status and education level • Loss of parent, sibling, or close friend • Stress related to adolescent developmental or issues of sexuality (eg, homosexuality)
Identifying Risk FactorsGenetic • Depressed parent contributes both genetic vulnerability & emotional unavailability that can contribute • combination of adverse life events and the presence of the shorter allelic form of the serotonin transporter gene results in early-onset depression • Smaller prefrontal cortex and basal ganglia in depressed individuals
Identifying Risk Factors • Medications • glucocorticoids, immunosuppressives, isotretinoin, antiviral agents • Chronic illness • such as cystic fibrosis, juvenile diabetes
DiagnosisThe Basic Steps • Are symptoms present? • Evaluate child’s current level of functioning relative to his or her baseline • Any potential for self-injurious behavior, suicidal ideation, or suicide attempt? • History taken from: • Patient • Parents • Others : teachers, counselors, or coaches.
DiagnosisTools • Children’s Depression Inventory (CDI) • assesses the severity of depression in prepubertal school-age children • Beck Depression Inventory (BDI) Reynolds Adolescent Depression Scale (RADS-2) • Mood and Feelings Questionnaire (MFQ) Adolescents
DiagnosisTools • The Guidelines for Adolescent Depression in Primary Care (GLAD-PC) Toolkit • Has child and parent report measures and scoring instructions on their web site http://www.thereachinstitute.org/files/documents/GLAD-PCToolkit.pdf • This user-friendly online resource also includes management flowcharts, scales, and educational materials in English and Spanish as well as tracking forms and information on billing
TreatmentPharmacological • Currently, fluoxetine (Prozac)is the only antidepressant approved by the FDA in children and adolescents • research studies have demonstrated efficacy of other drugs such as citalopram, paroxetine, and sertraline • Dosing of Fluoxetine • Starting at 2.5 mg/day for prepubertal children • 10 mg/day for older adolescents • Most patients respond to fluoxetine at doses ranging from 20 to 80 mg/day
TreatmentPharmacological • 2006 FDA meta-analysis of children and adolescents taking SSRIs for depression • found an increased risk of suicidality in those patients treated with drugs versus those given placebo. • Subsequent meta-analysis including additional studies revealed that those who benefited from SSRI treatment outnumbered those who became suicidal during SSRI treatment by a ratio of 14:1.