Download
1 / 24
310 likes | 757 Views
Thyroid gland. The normal circulating thyroid hormones are Thyroxine T4 (90%),Triiodothyronine T3 (9%) and rT3 (1%). Reverse T3 (rT3) is biologically inactive form of T3. Thyrotoxicosis or hyperthyroidism (Graves disease) is the clinical syndrome caused by an excess of thyroid hormones.

E N D
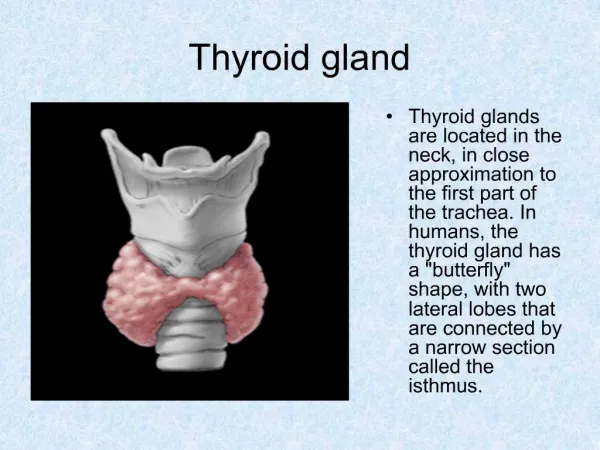
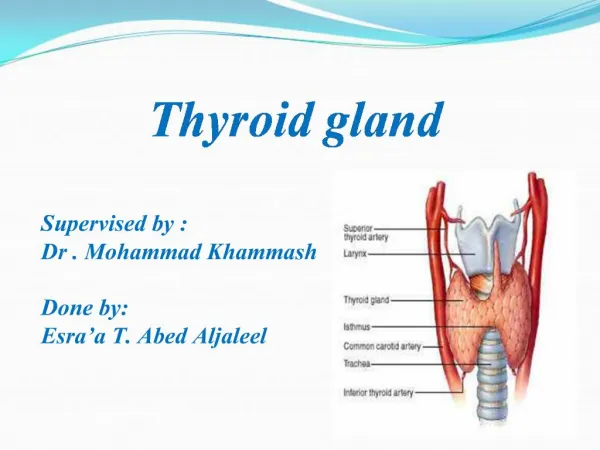
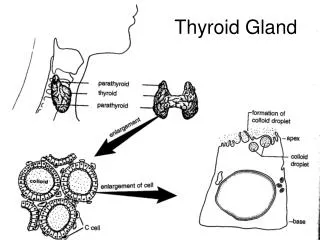
Thyroid gland • The normal circulating thyroid hormones are Thyroxine T4 (90%),Triiodothyronine T3 (9%) and rT3 (1%). • Reverse T3 (rT3)is biologically inactive form of T3. • Thyrotoxicosis or hyperthyroidism (Graves disease) is the clinical syndrome caused by an excess of thyroid hormones. • Hypothyroidism (Hashimoto's thyroiditis) is a clinical disorder in which there is a deficiency of thyroid hormones.
THYROID HORMONES Increases basal metabolic rate. Potentiates brain development. Potentiates the beta effects of catecholamines.
Thyroid gland Metabolism of thyroid hormones : • The primary metabolism of thyroxine is deiodination. • Deiodination of T4 may occur by monodeiodination of outer ring producing 3,5,3’- triiodothyronine - T3 ( T3 is 4 times more potent than T4) by 5’-monodeiodinase. • Deiodination of inner ring produce 3,3’,5’ – reverse triiodothyronine – rT3 (inactive) by 5-monodeiodinase.
Inner ring Outer ring 5’-monodeiodinase. 5-monodeiodinase.
Thyroid hormones Metabolism of Thyroid hormones : • Drugs like beta blockers, high dose propylthiouracil and steroid inhibit the 5’-deiodinase activity necessary for conversion of T4 to T3 resulting in low T3 and high of rT3.
Thyroid gland Mechanism of action of thyroid hormones : • T4 dissociate from thyroxine binding globulin in plasma before entry into cells. • In the cells, T4 is enzymatically deiodinated to T3 which enters nucleus and attaches to specific receptors which promotes protein synthesis.
Anti-thyroid drugs Drugs used for the treatment of hyperthyroidism : Inhibition of hormone synthesis : • Propylthiouracil and Methimazole. Blockade of hormone release : • Iodides, Iodinated contrast media. Radioactive Iodine 131 Anion Inhibitors : • Perchlorates, Thiocynates. Beta blocking drugs :Propranolol.
Anti-thyroid drugs peroxidase
Anti-thyroid agents THIOAMIDES : • Inhibit hormone synthesis by inhibitingperoxidase. • Propylthiouracil also inhibits peripheral deiodination of T4 and T3. • Methimazole is more potent and longer acting than propylthiouracil. • Slow in onset ~ 4 weeks.
Anti-thyroid drugs THIOAMIDES : • These are used for treatment of mild thyrotoxicosis and in preparation of surgery. • Propylthiouracil is relatively safe and preferred in pregnancy.
Anti-thyroid drugs THIOAMIDES : ADVERSE EFFECTS • Common adverse effects includes maculopapular rash, arthralgia and vasculitis. • Agranulocytosis – reversible.
Anti-thyroid drugs Potassium iodide : Inorganic iodide • It blocks the organification and release through inhibition of proteolysis – known as Wolff – Chaikoff effect. • It decrease the size and vascularity – used before surgery. • Rapid improvement in 2-5 days. • It is an ideal agent for the treatment of severe thyrotoxicosis and preoperatively.
Anti-thyroid drugs Potassium iodide : Inorganic iodide • Anti-thyroid effect is not for long term as gland ‘escapes’ from its effect. • This is the most effective way of limiting the potential damage to thyroid gland by radiation emergencies.
Anti-thyroid drugs Potassium iodide : Inorganic iodide • Chronic use in pregnancy avoided – fetal goiter. • Adverse reactions to iodine includes – iodine induced thyrotoxicosis (Jod Basedow’s phenomenon) at low doses. • Others includes – salivary gland inflammation and acne.
Anti-thyroid drugs Radioactive Iodine : • I-131 is the only isotope used in treatment of thyrotoxicosis while others are used in diagnosis. • Administered as sodium I–131 orally. • Therapeutic effect depends on emission of beta rays – destroys the thyroid gland. • Patients eventually becomes hypothyroid – managed with thyroxine.
Anti-thyroid drugs Radioactive Iodine : • I–131 serves as alternative to surgery. • Easy, effective, low cost and absence of pain are the advantages. • Not advisable for pregnant women.
Anti-thyroid drugs ANION INHIBITORS : • Monovalent ions like perchlorate, pertechnetate, thiocyanate can competitively block the uptake of iodine. • Anion inhibitors are uncommon in use because of aplastic anemia. • These are effective in iodine induced hyperthyroidism
Anti-thyroid drugs Iodinated contrast media : Diatrizoate / Iohexol : • They are valuable in hyperthyroidism and as adjunctive in thyroid storm. • They inhibit the peripheral conversion of T4 into T3. • Inhibition of hormone release is an additional mechanism.
Anti-thyroid drugs Other Anti-thyroid drugs : • Propranolol isused in the management of cardiac symptoms of thyrotoxicosis. • Lithium is known to inhibit synthesis and release of thyroid hormones. • Amiodaronecan also result in hypothyroidism.
Thyroid gland • The extreme manifestations of untreated hypothyroidism is myxedema coma with a mortality ~ 50%. • Myxedema coma is treated with intravenous T4 or sometimes T3. • Levothyroxine T4 is the best choice for replacement therapy. • Thyroid hormones replacement is monitored by plasma TSH.
Thyroid gland Thyroid storm: Thyrotoxic crisis, is an acute, life-threatening state induced by excessive release of thyroid hormones. • Propranolol to minimize cardiac symptoms • High-dose propylthiouracil is preferred because of its ability to inhibit peripheral conversion of T4 to T3 • Potassium iodide used to block the release of thyroid hormones