Download
1 / 51
570 likes | 984 Views
Laparoscopic Ventral Hernia: avoiding and managing complications. Brian Jacob MD FACS. Synthetic mesh will react like a foreign body. Fibrous ingrowth into mesh Strength may peak between 4 – 12 weeks* May incite chronic inflammatory response ↑ Rigidity ↓ Elasticity ↓ Compliance

E N D
Laparoscopic Ventral Hernia: avoiding and managing complications Brian Jacob MD FACS
Synthetic mesh will react like a foreign body Fibrous ingrowth into mesh Strength may peak between 4 – 12 weeks* May incite chronic inflammatory response ↑ Rigidity ↓ Elasticity ↓ Compliance Nerve entrapment or inflammation / irritation *Majercik S, Tsikitis V, Iannitti DA (2006) Strength of tissue attachment to mesh after ventral hernia repair with synthetic composite mesh in a porcine model. Surg Endosc. 20(11):1671-4
Mesh can lose compliance Courtesy Dr. Bruce Ramshaw
Mesh shrinks Video clip of shrunken mesh
Mesh can get infected Courtesy Dr. Ramshaw
“never judge the laparoscopic surgeon until you have seen him or her do a laparoscopic ventral hernia repair.”
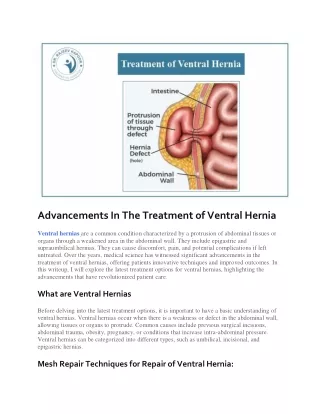
What we don’t want: • Bowel can adhere to polyester surface • Inadequate overlap • Inadequate fixation
Safe Adhesiolysis • Sharp dissection if bowel involved • Important to get all of the contents reduced Video clip of adhesiolysis
Reduce all hernia contents • Sharp dissection if bowel involved • Important to get all of the contents reduced • Small defects can contain a lot of incarcerated omentum
Measuring the defect • Draw on abdomen • Needles • Use a ruler
Pole the audience • During a laparoscopic ventral hernia for a small to medium-sized defect, in addition to inserting mesh with good overlap, do you believe there is a benefit to also closing the defect?
Closing the defect:(small or large ones) • May limit seroma formation • Less mesh bulging in larger defects • Limits mesh exposure to infection
LVHR: Closing the defect • No randomized data exists in laparoscopic ventral hernia literature • More anatomic and physiologic (wound healing) • May limit morbidity (seroma) • Larger sized defects: may offer cosmetic and functional benefits • Less bulging (known morbidity) • Benefit in initiating the wound healing process?
Closing the defect : consider lap component separation as needed Video clip of lap component separation
Surgical Technique:Mesh Selection and Preparation • Measure defect • Select mesh with at least 4cm overlap if possible • Map out your plan on abdomen • Use letters to mark transfascial fixation points • Prepare mesh with sutures for transfascial fixation
Surgical Technique:Securing of Mesh • Make small skin incision with 11 blade scalpel • Bring 2 ends through individually using needle-type suture passer
Wound and Mesh Complications • N = 3276 (19 articles with >50 pts) • Seroma (11.4%) • Mesh Infection (0.6%) • Wound Infection (1.1%) • Fistula (0.1%) Cobb WS, Kercher KW, and Heniford BT 2005 Surg Clin N Am 91-103
Other associated risks of laparoscopic ventral hernia repair • Ileus (2-3%) • Enterotomy (1.8%) • Identified and repaired (80%) • Missed (20%) • Increases mortality rate to 7.7% • Acute Pain (99%) • “Forewarned is forearmed” • Chronic pain (1.6%) • Suture and tack removal may only help some patients LeBlanc KA, Elieson MJ, Corder JM, Enterotomy and mortality rates of laparoscopic incisional and ventral hernia repair: a review of the literature JSLS 2007 Oct-Dec;11(4):408-14
Bleeding after tacking • Video clip
Morbidities: Seroma / Hematoma • Incidence • 5 - 12 % • Management • Conservative • Postpone aspiration as long as possible
Mechanisms of enterotomy • Immediate injury • Trocar • Adhesiolysis • Delayed injury • Thermal burn • Cautery • Ultrasonic shears
Mechanisms of enterotomy • Video clip
Morbidities: Recurrence • Incidence • 0 – 9% • Management • Case specific
Recurrence • Literature • Video clip
Morbidities: Wound / Mesh Infection • Incidence • 2 – 5.6% • Management • Perc drains • ?antibiotic irrigations • Mesh removal
Foreign Body:Biofilm • Bacteria adhere to mesh fibers • Lay down a biofilm • Protect bacteria from host immune system • Bacteria survive • Chronic infections • Material used doesn’t matter!!
Biocompatibility of bacterial contaminated prosthetic meshes and porcine dermal collagen used to repair abdominal wall defects • 96 rats • N = 12 (sterile and contaminated) • PPM • PPM with titanium • Polygylcol (absorbable) • Porcine dermal collagen (biologic) Ott R et al. Germany. Langenbecks Arch Surg. 2007
Mesh and Infection Don’t Mix Well • Independent of type, all mesh was infected at 28 days • Infected mesh intra-abdominally can lead to more adhesions and even fistulas • Insertion of biologic mesh into an infected field can become infected Ott R etal. Biocompatibility of bacterial contaminated prosthetic meshes and porcine dermal collagen used to repair abdominal wall defects Germany. Langenbecks Arch Surg. 2007
Despite material, know when your routine laparoscopic repair isn’t going to be enough
LVHR: When should I say “no”? • Limitations: • Very large defects that might require component separation • Significant intraabdominal adhesions • Eroding mesh to skin • Other complex hernias
Combined open component separation with laparoscopic mesh fixation
Patient Selection: Identifying a tough patient YES TOUGH PATIENT Risk for recurrence? Obesity Diabetes COPD and smoking history Malnutrition Steroids Radiation history Abnormal collagen metabolism YES Risk for mesh infection? Large Immunocompromised Fistula in the past Infectious diseases Clean contaminated cases No No Routine Hernia Repair with mesh Defect Size? Small
Recurrence risk Infection risk Large Defect Tough Patient • Bowel Resections • Cholecystectomy • Enterotomy • Enteroentero Fistulas • Inflammatory Bowel Cases • Appendectomy Is this also a Complex Hernia? Atypical Hernia Location Loss of Domain Giant Defects ( >10cm) Active Infections (Contaminated Case) Potential Infections (Clean contaminated) • Mesh Infections • Colocutaneous fistulas • Perforations • Peritonitis NO Routine Hernia Repair If Yes, then……
Abdominal Wall Reconstruction: grossly infected or contaminated hernia • Stoppa or Component separation • No mesh vs biologic vs absorbable • Staged operations • Progressive preoperative pneumoperitoneum • ePTFE serial excision (silo) • Free tissue flaps
Conclusions: keys to success • Laparoscopic ventral hernia • Low morbidity • Reproducible technique that should be adhered to • Defects and patients are NOT created equal • Choose the right procedure and product for each patient