Download
1 / 94
940 likes | 967 Views
Biology 220 Anatomy & Physiology I. Unit XI ENDOCRINE SYSTEM. Chapter 17, pp. 608-649. E. Gorski/ E. Lathrop-Davis/ S. Kabrhel. Nervous. Endocrine. messenger. electrochemical. hormone (chemical). response. milliseconds. seconds to days. duration. short-lived. long-lived.

E N D
Biology 220 Anatomy & Physiology I Unit XIENDOCRINE SYSTEM Chapter 17, pp. 608-649 E. Gorski/ E. Lathrop-Davis/ S. Kabrhel
Nervous Endocrine messenger electrochemical hormone (chemical) response milliseconds seconds to days duration short-lived long-lived distribution one system (several subsystems) widely scattered Comparison of Nervous and Endocrine Systems NOTE: Nervous and endocrine systems work together to coordinate and integrate activities of body (homeostasis)
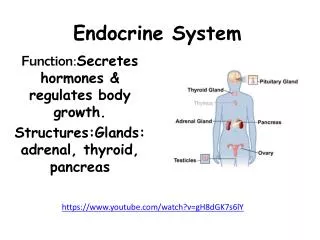
Functions of Endocrine System 1. Reproduction 2. Growth and development 3. Response to stress 4. Maintenance of fluid (water), electrolyte and nutrient balance 5. Regulation of cellular metabolism and energy
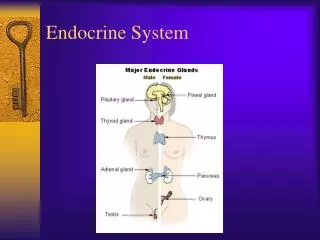
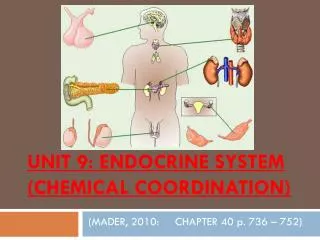
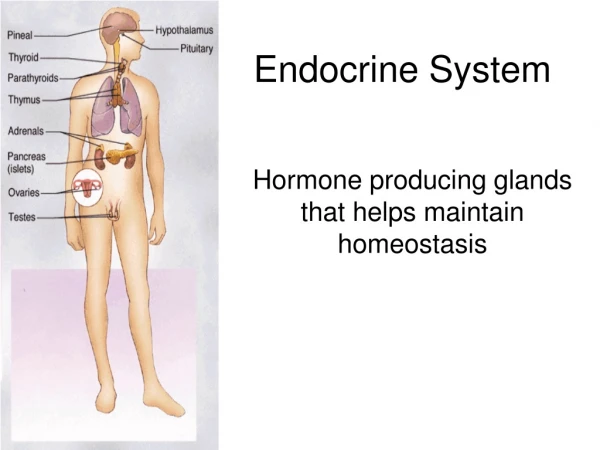
Organs of the Endocrine System 1. Pituitary gland 2. Hypothalamus (neuroendocrine) 3. Pineal gland 4. Thyroid gland 5. Parathyroid gland 6. Thymus gland 7. Adrenal gland 8. Pancreas (also has exocrine function) 9. Gonads (testes or ovaries - also have exocrine functions) Fig. 17.4, p.616
Topics • Hormone • Types • Modes of Action • Target cell activation • Control • Specific glands, their hormones, and disorders • Pituitary • Thyroid • Parathyroid • Adrenal • Pancreas • Thymus • Gonads (testes and ovaries) • General Adaptation Syndrome
Hormones • chemicals • secreted by endocrine gland cells into blood (by way of interstitial fluid) • regulate metabolic functions of other cells (called target cells) • carried to all cells, but action is specific to cells that have receptors for the hormone • specificity of body’s response to hormone depends on how many cells have the receptor (highly specific if few cells respond [e.g., ACTH]; diffuse action if many respond [e.g., thyroxine])
Chemical Types of Hormones • Amino-acid based (amino acids, short or long peptides, proteins) • e.g., insulin, growth hormone, prolactin • Steroids - lipid derivatives of cholesterol • e.g., hormones from gonads (testosterone, estrogen) • e.g., hormones from adrenal cortex (adrenocortical hormones) • Eicosanoids - locally-secreted, locally-acting hormones secreted by all cell membranes (e.g., prostaglandins, which increase blood pressure and contribute to uterine contraction)
Types of Changes in Target Cells • plasma membrane permeability changes (opening of protein channels; may change membrane potential) • activation of genes for increased protein synthesis, including enzymes • activation or deactivation of enzymes already present • secretion of cellular products • stimulation of cell division (mitosis)
Mechanisms of Action • action in target cell depends on receptor • receptor may be: • in plasma membrane • second messenger mechanisms • used by most amino acid-based hormones (water soluble) • intracellular (in cytoplasm or nucleus) • direct gene activation • used by steroids and thyroid hormones (lipid soluble)
Mechanisms of Action: Steroids • bind tointracellular receptors • hormone diffuses through plasma membrane and makes its way to nucleus • > where it binds with intracellular receptor to form hormone-receptor complex • > hormone-receptor complex interacts with chromatin (DNA) to affect gene activity (turn genes on or off) • > synthesis of mRNA • > synthesis of protein
Steroid Signaling Fig. 17.2, p. 613
Mechanism of Action:Thyroid Hormone • similar to mechanism for steroid hormones • diffuses across plasma membrane • diffuses into nucleus where it interacts with intracellular receptors to activate genes for proteins (enzymes) involved in cellular respiration (glycolysis) • also, binds to receptors at mitochondria to activate genes for proteins involved in cellular respiration (Krebs cycle and electron transport chain)
Mechanisms of Action: Other Hormones • plasma membrane receptor • used by most amino acid-based hormones • interaction of hormone with plasma membrane receptor results in activation of second messengersystems (cyclic AMP or PIP-calcium) • activation of second messenger has cascade effect resulting in: • enzyme activation, or • membrane permeability changes or secretion
Membrane Receptor Mechanisms:1. Cyclic AMP (cAMP) Signaling • interaction of hormone with receptor • > activates G protein (cleaves phosphate from GTP)-> excitation • > G protein activates adenylate cyclase • > adenylate cyclase forms cAMP from ATP • > cAMP activates protein kinases • > protein kinases activate (or inhibit) other proteins by phosphorylation • > cAMP degraded by enzyme • slightly different G protein inactivates adenylate cyclase - associated with different hormone receptor • Link to animation: http://student.ccbc.cc.md.us/c_anatomy/animat/cAMP.htm
cAMP Signaling Mechanism Fig. 17.1, p. 611
Membrane Receptor Mechanisms:2. PIP-Calcium Signaling • interaction of hormone with receptor --> activates membrane-bound enzyme phospholipase • > phospholipase cleaves PIP2 (phosphatidyl inositol diphosphate) into diacylglycerol(DAG) and IP3 -- each of which acts as a second messenger • diacylglycerol (DAG) activates protein kinases • IP3 (inositol triphosphate) causes release of Ca2+ into cytoplasm (from endoplasmic reticulum or other storage areas) --> Ca2+acts as third messenger
PIP-Calcium Mechanism (con’t) -> Ca2+ (third messenger) • changes enzyme activity and plasma membrane channels, or • binds to calmodulin (intracellular regulatory protein) --> activates enzymes • see Fig. 17.2 for examples of proteins that act through membrane-receptors and 2nd messengers
PIP-Calcium Signaling Mechanism Fig. 17.1, p. 612
Factors Affecting Target Cell Activation a. blood levelsof hormone, which depend on: • rate of hormone release • rate of deactivation (by target cell or liver) b. affinityof hormone for receptor • greater affinity means greater association --> greater effect c. number of receptors available
Factors Affecting Target Cell Activation (con’t) c. number of receptors available • up-regulation: increase in blood level of specific hormone (normally present at low levels) causes cells to make more receptors • down-regulation: prolonged exposure to high level of specific hormone --> cells remove some receptors -->return to normal response level • cross-regulation: influence of one hormone on number of receptors for another hormone; e.g., progesterone causes uterus to make fewer estrogen receptors; estrogen causes uterus to make more progesterone receptors
Hormone Removal • hormones may be: • degraded by specific enzymes within target cells; • removed from blood by kidneys (excreted in urine) • degraded by liver (excreted in urine and feces) • half-life - time for 1/2 of hormone to be removed (from a fraction of a minute to 30 minutes) • onset - time from release to action (minutes [amino acid-based] to days [steroids]) • duration of action - how long the effects last (~20 minutes to several hours)
Control of Hormone Release • Humoral control • Neural control • Hormonal control
Control of Hormone Release: Humoral Hormone released in response to changing blood levels of ion or nutrient (negative feedback) parathyroid glands: detects low blood Ca2+ PTH raises blood Ca2 thyroid (parafollicular cells) detect high blood Ca2+-->calcitonin-->decrease blood Ca2+ Fig.17.3, p615
Control of Hormone Release: Humoral Other examples: • pancreas: • beta cells detect high blood glucose insulin decreases blood glucose • alpha cells detect low blood glucose glucagon raises blood glucose • zona glomerulosa (of adrenal cortex) detects low blood Na+ or high blood K+ aldosteronetthy, K+
Control of Hormone Release: Neural Hormone released in response to nerve impulse preganglionic fibers of sympathetic division stimulate release of catecholamines (epinephrine, norepinephrine) from adrenal medulla impulses from hypothalamus result in release of oxytocin or ADH from posterior pituitary Fig. 17.3, p. 615 Fig. 17.5, p. 617
Control of Hormone Release: Hormonal Hormone produced by one endocrine gland (or hypothalamus) affects secretion of hormone by another endocrine gland • hypothalamus acts as overall coordinator releases regulatory hormones (releasing hormones or inhibitory hormones) affects anterior pituitary • anterior pituitary, when stimulated,secretes hormones that affect other glands (e.g., TSH [thyroid stimulating hormone] stimulates release of thyroid hormones from thyroid gland)
Hormonal Control: Role of Hypothalamus • Releasing hormones from hypothalamus stimulate secretion from anterior pituitary • Inhibitory hormones from hypothalamus inhibit secretion by anterior pituitary • Impulses from hypothalamus cause release of hormones from posterior pituitary Fig. 17.5, p. 617
Hormone Control - Misc. • nervous system can override normal endocrine control • e.g., in “fight-or-flight” response, sympathetic impulses result in release of epinephrine and norepinephrine from adrenal medulla --> increases blood glucose levels to maintain fuel supply during stress or exertion (overrules effect of insulin on blood glucose level)
Organs of the Endocrine System and Their Products • The following major glands will be covered one at a time with their products: 1. Pituitary gland / Hypothalamus 2. Thyroid gland 3. Parathyroid gland 4. Adrenal gland 5. Pancreas (also has exocrine function) 6. Gonadal hormones (ovaries and testes) 7. Thymus Fig. 17.4, p. 616
1. Pituitary Gland (Hypophysis) • located in sella turcica of sphenoid bone (in cranial cavity), inferior to hypothalamus • consists of two lobes: A. neurohypophysis (~ posterior pituitary) • attached to hypothalamus by infundibulum • contains axons and axon terminals of neurosecretory cells whose cell bodies are in hypothalamic nuclei B. adenohypophysis (~ anterior pituitary) • consists of glandular epithelium http://www.usc.edu/hsc/dental/ghisto/end/c_1.html
Pituitary Development From roof of mouth http://calloso.med.mun.ca/~tscott/head/pit.htm
A. Neurohypophysis (Posterior Pituitary) • consists of nerve fibers (axons of neurosecretory cells with cell bodies in hypothalamus) and pituicytes (glial cells that support nerve fibers) • acts primarily as a storage and releasing area for hormones actually made in hypothalamic nuclei • hormones released in response to impulses from hypothalamus (neural control) • hormones are short amino acid chains (peptides) • oxytocin • antidiuretic hormone (ADH or “vasopressin”)
A. Neurohypophysis:Oxytocin (OT) • action, in pregnant or nursing women: • stimulates contraction of smooth muscle of uterine wall during labor and delivery • stimulates ejection of milk in lactating mothers • action, in men and non-pregnant women, may be involved in sexual arousal and orgasm
A. Neurohypophysis:Oxytocin (OT) • control: • during labor/delivery, positive feedback: stretching of uterus/cervix --> sensory impulses to hypothalamus --> increased secretion of OT --> increased contraction • suckling: sucking of infant on breast --> sensory to hypothalamus --> oxytocin release --> release of milk
A. Neurohypophysis: Antidiuretic Hormone (ADH) • action: antidiuretic hormone (ADH) directly affects blood pressure - acts as powerful vasoconstrictor --> increases blood pressure (hence name “vasopressin”) • action: affects water balance (indirect affect on blood pressure) - acts on tubules of kidney to increase reabsorption of water less water lost in urine
A. Neurohypophysis: ADH • disorders: • hyposecretion due to damage of hypothalamic nucleus or neurohypophysis--> diabetes insipidus - excessive urine production (polyuria) and thirst • hypersecretion --> SIADH (syndrome of inappropriate ADH secretion) - water retention, headache, cerebral edema, weight gain, hypoosmolarity
Antidiuretic Hormone (ADH): Control • neural control: increased electrolyte (NaCl) concentration --> affects (supraoptic) nucleus in hypothalamus --> impulse to neurohypophysis --> release of ADH --> increased water reabsorption --> decrease in electrolyte concentration • other stimuli: pain, low BP, morphine, barbiturates, nicotine, aldosterone (hormone from adrenal cortex - hormonal control) • inhibition: alcohol (results in more urine production and, potentially, dehydration) • diuretic drugs - some act to supress ADH secretion; used to treat hypertension and congestive heart failure
B. Adenohypophysis (Anterior Pituitary) • linked to hypothalamus via hypophyseal portal system (capillary networks and small veins) • carries regulatory hormones from hypothalamus to pituitary • releasing hormones stimulate secretion of pituitary hormones • inhibitory hormones inhibit secretion • consists of epithelial cells • all hormones produced are proteins • tropic hormones - affect some endocrine glands or provide maintenance oversight for other organs
B. Adenohypophysis:Growth Hormone (GH) • highest levels during evening and sleep • action: stimulates increased rate of protein synthesis leading to cell growth and division • bones and skeletal muscle respond more than other body cells • action: stimulates use of fat as energy source and decreases rate of glucose uptake and glucose metabolism (diabetogenic effect – “spares” glucose) • control: • release stimulated by GHRH (growth hormone releasing hormone) from hypothalamus • inhibited by GHIH (from hypothalamus) and somatomedins (produced by liver under GH stimulation)
Growth Hormone (GH): Disorders Disorders: • hypersecretion • gigantism (in children) • up to 8’ tall, normal body proportions • acromegaly (after epiphyseal plates close) • enlargement of extremities and face, thickening of soft tissue • hyposecretion • pituitary dwarfism - in children, up to 4’ tall • progeria - premature aging, atrophy of body tissues *See Fig. 17.6, p. 619
B. Adenohypophysis: Prolactin (PRL) • action: • stimulates milk production in mammary glands; • helps stimulate development of mammary glands (along with other hormones); • in males, may help regulate testosterone production • control: • stimulation: PRH (prolactin-releasing hormone from hypothalamus), high estrogens, breast-feeding • inhibition: PIH (hypothalamus), stimulated by rising PRL levels, low estrogen
B. Adenohypophysis:Prolactin (PRL) Disorders • hyperprolactinemia = hypersecretion due to adenohypophyseal tumors; results in galactorrhea, lack of menses and infertility in women, impotence in men
B. Adenohypophysis: Thyroid-Stimulating Hormone (TSH) • TSH = thyrotropin • action: • stimulates secretion of hormones from thyroid gland (T4 and T3); also stimulates development of thyroid in youth • control: • release stimulated by TRH (thyroid releasing hormone from hypothalamus) • inhibited by rising levels of thyroid hormones and by GHIH
B. Adenohypophysis: Adrenocorticotropic hormone (ACTH) • ACTH=corticotropin • action: stimulates release of hormones from adrenal cortex • control: • release stimulated by CRH (corticotropin-releasing hormone from hypothalamus) • release inhibited by rising levels of glucocorticoids from adrenal cortex
B. Adenohypophysis:Gonadotropins • regulate activity and secretion by gonads (testes in males; ovaries in females) • control: • stimulated by GnRH (gonadotropin-releasing hormone from hypothalamus) • release of GnRH is inhibited by rising levels of estrogens, progestins and androgens (testosterone) • two important hormones • FSH • LH
Gonadotropins:Follicle-Stimulating Hormone (FSH) • action: • females (ovaries) - stimulates development of ovarian follicles and estrogen production • males (testes) - stimulates sperm production and development • inhibited by inhibin and testosterone from testes (feedback to hypothalamus and anterior pituitary) and estrogen, progesterone and inhibin from ovaries (feedback to anterior pituitary)
Gonadotropins:Luteinizing Hormone (LH) • LH=lutropin • action: • females (ovaries) - induces ovulation; stimulates secretion of estrogens and progestins (e.g., progesterone) • males (testes) - stimulates production of androgens (e.g., testosterone ) • inhibited by estrogen, progesterone and inhibin form ovaries (feedback to anterior pituitary) and by inhibin and testosterone from testes (feedback to hypothalamus and anterior pituitary)
2. Thyroid Gland • located anteriorly in cervical region, just inferior to thyroid cartilage; two lobes connected by thin isthmus • largest purely endocrine gland in body • consists of follicles (cuboidal or simple squamous epithelium) filled with colloid (combination of protein [thyroglobulin] containing amino acid tyrosine [building block of thyroid hormones]) • parafollicular cells produce calcitonin http://www.usc.edu/hsc/dental/ghisto/end/c_26.html
2. Thyroid Gland: T4 and T3 • hormones based on amino acid tyrosine (differ in number of iodine ions) • thyroxine (tetraiodothyronine [T4]) and • triiodothyronine (T3) • T3 is 10x more active, but less common (T4 accounts for about 90% of all thyroid hormone) • much T4 converted to T3 by liver, kidneys, some other tissues
2. Thyroid Gland: T4 and T3 • affect metabolic rate of every cell in the body, except brain, spleen, testes, uterus and thyroid gland • affect other activities within these organs and glands • readily cross membranes (diffuse through plasma membrane to bind to mitochondrial receptors and receptors in nucleus)