Download
1 / 31
1.79k likes | 7.32k Views
Intestinal Tuberculosis. Second Affiliated hospital Yan Chen. Intestinal tuberculosis. General situation Etiology and pathogenesis Pathology Clinical manifestation lab & other examination Diagnosis and differential diagnosis Treatment , prognosis and prevention. General ideas.

E N D
Intestinal Tuberculosis Second Affiliated hospital Yan Chen
Intestinal tuberculosis • General situation • Etiology and pathogenesis • Pathology • Clinical manifestation • lab & other examination • Diagnosis and differential diagnosis • Treatment , prognosis and prevention
General ideas • Developing countries (95%), especially poverty, malnutrition, overcrowding and HIV coinfection. • Involvement of intestine is usually secondary to pulmonary tuberculosis.
The ileocecal region is the most common area of involvement in the intestinal tract . Why ? • The abundance of lymphoid tissue • Long residence time of bactera in ileocucum
Predisposing factors • Fatigue • poor sanitation • malnutrition • lowered resistance etc.
Pathogenic organism----tubercle bacillus • tubercle bacillus maybe either the human type or bovine type human type----90% bovine type----10%
Etiology and pathogenesis Route of transmission • Propagation by mouth: • Hemotogenous dissemination: miliary TB • Spread straightly:
Etiology and pathogenesis • Bacilium: number, virulence • Decreased immunity of human • Weakening of intestinal resistance
Clinicalmanifestation Local symptoms ●abdominal distension ● ascites ● mass ●abdominal pain ● diarrhea & constipation ● complication Systemic symptoms ● Fatigue ● low-grade fever ● Night sweats ● Loss of weight ● poor appetite ● anemia Extraintestinal tuberculosis manifestation : pulmanory TB
laboratory findings • erythrocyte sedimentation rate, ESR ●ESRtypically elevated in the active stage ● Stool routine test : occult blood
laboratory findings • PPD test purified protein derivative tuberculin skin test • culture or histological examination of specimen • biopsy-microscopic tissue exam revealed tubercular histological feature of TB
Radiography • In advanced cases, symmetric annular stenosis and obstruction associated with shortening, retraction, and pouch formation may be seen. The cecum becomes conical, shrunken, and retracted out of the iliac fossa due to fibrosis within the mesocolon, Ileocecal valve becomes fixed, irregular, gaping, and incompeten Straight arrow show Conical and shrunken cecum;curved arrow show the narrowing of the terminal ileum
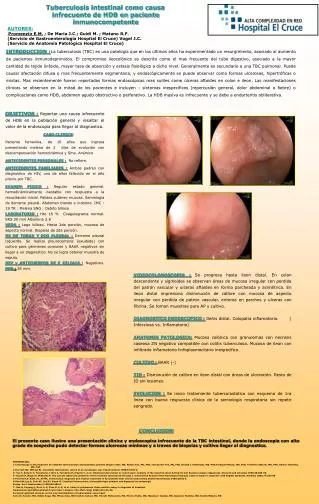
Colonoscopy TB
Colonoscopy Ulceration
Imaging features Ultrasonography, CT, MRI • Asymmetric bowel wall thickening • Ascites • Inflammatory mass of bowel wall • Narrowing of the terminal ileum with thickening and gaping of the iliocaecal valve • Fluid surrounding bowel caused by inflammation of the bowel wall
Other examinations • Laparoscopic biopsy of tubercles found in the peritoneum or other parts • Laparotomy • Capsule endoscopy • enteroscopy
Diagnosis & differential diagnosis Diagnostic criteria • Younger patients presented with extraintestinal TB • Symptom: toxic symptom diarrhea, abdominal pain, abdominal mass • X-ray: sterlin sign, stricture of bowel, deformation • Colonoscopy and biopsy: inflammation,ulcer,polyp,striction caseating granuloma, bacterium(+) • PPD test :strongly positive • Exploratory laparotomyfor patients difficult to be diagnosed • Experimental treatment :2-8 weeks
Diagnosis & differential diagnosis Differential diagnosis • Crohn’s disease: The major diagnostic dilemma of ITB is to differentiate it from CD. • Right-sided colonic carcinoma • Amoebiasis or schistosomicgranuloma • Chronic bacillary Dysentery or cholera • Malignant lymphoma • FGID:IBS, functional diarrhea
TB & CD TB CD • Extraintestinal TB √ • Course(relief and relapse) √ • Fistula/abscess/peri-anal lesion √ • Segmental appearance √ • Form of ulcer transverse longitudinal • Caseating granuloma by biopsy √ • PPD test with strong positive √ • Effective Anti-TB treatment √
The ileocecal region • Female • years old • Right lower quadrant pain and fever Sigmoid and Rectom
Treatment • purpose: resolve symptom, improve constitutional condition, promote curing, prevent complication • Measures: rest nutritional support anti-TB chemotherapy relieve symptom surgery
tuberculous peritonitis • Same as tuberculous pleurisy