Download
1 / 29
300 likes | 705 Views
Surgical Airway—the last strategy in airway management . Presented by Kang, Ting-jui. CASE ( I ) . Brief History. 57 y/o female with NPC s/p radiotherapy Denied any other systemic disease One episode of massive bleeding from nose and oral cavity on 2/7 Vital sign stable, consciousness clear

E N D
Surgical Airway—the last strategy in airway management Presented by Kang, Ting-jui
Brief History • 57 y/o female with NPC s/p radiotherapy • Denied any other systemic disease • One episode of massive bleeding from nose and oral cavity on 2/7 • Vital sign stable, consciousness clear • Anterior packing with V-G and posterior packing with Foley catheter for stopping bleeding
Intra-operation • Tracheostomy and TAE were suggested • Emergent tracheostomy was initiated in OR under local anesthesia • ENT doctor asked us of setting ventilator after tracheostomy was inserted • De-saturation and consciousness loss was noted when we arrived • High pressure while resuscitation bagging, capnography showed no end-tidal concentrations of CO2
Intra-operation • The suction tube can’t be passing through the tracheostomy tube • Tube mal-positioning was suspected and the ENT doctors kept trying to insert the tube • Saturation below 60% and downward in seconds • Bredycardia atropine 1mg was given • Trismus fiberoptic nasal intubation was performed • Standstill CPR start, bosmin and cardiac massage ROSC in 5 minutes send to SICU
CXR • Normal heart size.Bilateral pneumothorax and diffuse subcutaneous emphysema.Endotracheal tube with the tip above the carina
CXR • Normal heart size • Clear lung field.no significant pneumothorax • Diffuse subcutaneous emphysema from the bilateral neck to the abdominal wall • Bilateral chest tube • Endotracheal tube with the tip above the carina
Outcome • On arriving SICU, deep coma with loss of light reflex was noted • CXR showed diffuse subcutaneous emphysema and bilateral pneumothorax bilateral chest tubes were inserted • Next day (2/8), pupils returned to 2.0mm with positive light reflex and stable vital signs without any inotropic agent • Anisocoria was noted in the early morning of 2/10
Outcome • Brain CT showed severe brain swelling, blunting of cortex-white matter junction, cistern and sulci effacement and brain stem compression • Hypoxic encephalopathy was impressed. Cushing triad develped gradually and DI appeared • The patient died of brain death at 10:00AM on 2005/2/11
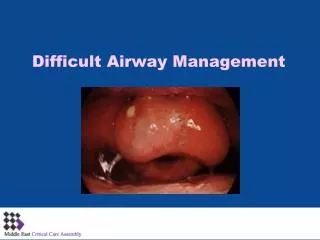
Review and Discussion • What did / should we do in this situation? • Apnea under local anesthesia in a related healthy person?
Brief History • 62 y/o male patient with NPC, T4N3aM0, Stage 4b s/p CCRT • Recurrence posterior pharyngeal tumor s/p excision and chemotherapy • He suffered from choking while oral intake • Consciousness drowsy with unstable hemodynamics • He was brought to our ER on 2/27 in the evening
CXR • Normal heart size with calcification of tortuous aorta. • Irregular and lobulated consolidation over the right mid-to lower lung field with blunting of right CP angle • Increased lung marking on both sides with some peribronchial infiltrations over the right perihilar and left lung field
Intra-operation • Aspiration pneumonia with sepsis was impressed • Establishing a patent airway was indicated due to easily choking, consciousness drowsy, oxygenation improvement, correction of metabolic and respiratory acidosis, aggressive chest care • Difficult intubation was noted the ER doctor consulted us and ENT doctors for airway management fiberoptic guide intubation “or” tracheostomy • Awake fiberoptic nasal intubation was performed smoothly in OR
Intra-operation • After intubation, the tracheostomy went on • Unfortunately, mal-position of the tracheostomy tube happened again!! • Tube exchanger guiding failed • Endotracheal tube advanced again cuff ruptured failed ventilation • Rapid desaturation and then asystole replace a new ETT via tube exchanger and CPR ROSC • Fiberoptic guide to insert the tracheostomy tube • Send the patient to ICU under high doses of inotropic agents
Outcome • In trauma ICU, poor saturation around 80% under 100% O2 and gradually downhill • Hemodynamic unstable under inotropics • Asystole on 2/28 in the early morning, CPR for 30 minutes but in vain
CXR • S/P tracheostomy. Pneumothorax and pneumomediastinum with mild subcutaneous emphysema over the left lower neck, supraclavicular area and upper chest wall • Massive pleural effusion on right side with passive atelectasis of the right lung, R/O hemothorax • Increased lung marking with prominent peribronchial infiltration on both sides
Review and Discussion • Was tracheostomy the necessary procedure for the patient in this situation? • Could we reacted better when tracheostomy tube mal-positioning? • What was the important diagnosis we missing?
Complications of Tracheostomy • Immediate (at the termination of the operation) • Apnea due to loss of hypoxic stimulation of respiration • Hemorrhage • Surgical injury of neighboring structures, i.e. esophagus, recurrent laryngeal nerve, and cupula of the pleura • Pneumothorax and pneumomediastinum • Injury of the cricoid cartilage (high tracheostomy)
Complications of Tracheostomy • Intermediate (the first few hours or days) • Tracheitis and tracheobronchitis • Tracheal erosion and hemorrhage • Hypercapnia • Atelectasis • Displacement of the tracheostomy tube • Obstruction of the tracheostomy tube • Subcutaneous emphysema • Aspiration and lung abscess
Complications of Tracheostomy • Late (for a prolong period) • Persistent tracheocutaneous fistula • Stenosis of the larynx or trachea • Tracheal granulations • Tracheomalacia • Difficult decannulation • Tracheoesophageal fistula • Problem with the tracheostomy scar