Download
1 / 36
360 likes | 600 Views
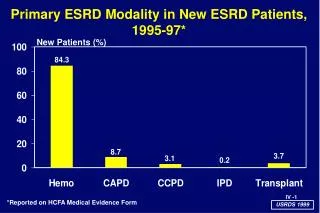
The New ESRD Regulations From the Surveyors Perspective. Liza Ben Vaughn, RN KDHE BCCHF QI Coordinator. ESRD Survey Focus. Protect Patient Safety and Improve Patient Outcomes Data is used to focus surveys Standards are incorporated into regulations (AAMI, CDC and NFPA)

E N D
The New ESRD Regulations From the Surveyors Perspective Liza Ben Vaughn, RN KDHE BCCHF QI Coordinator
ESRD Survey Focus • Protect Patient Safety and Improve Patient Outcomes • Data is used to focus surveys • Standards are incorporated into regulations (AAMI, CDC and NFPA) • Multiple resources for Standards
Resources for Standards • Regulations and Guidelines • FDA, NKF, NQF, American Nephrology Nurses’ Association, Renal Physicians Association • Manufacturer’s Directions • State Practice Acts • MAT (Measures Assessment Tool)
Focused Basic Survey Process • Initials • Complaints • Relocations • Change in service
STAR • Surveyor Technical Assistant for Renal Disease • An automated survey guide • Uses a wireless tablet PC • Guides the surveyor through the process • Roll out in some states. Kansas and Iowa are using STAR.
Sixteen Survey Tasks • Pre-survey • Introductions • Tour/Observations • Entrance conference • Patient sample selection • Water treatment-Dialysis preparation • Reprocessing-Reuse • Machine operation-maintenance • Home training department review
Patient interviews • Medical record reviews • Personnel interviews • QAPI • Personnel record reviews • Decision Making • Exit conference
“FLASH SURVEY” • Waiting room • Patient restrooms • Reuse room • Water-Dialysate areas • Home training area • Treatment area • Isolation
Observations and Tour • Ongoing throughout the survey • Physical environment • Infection control • Patient – Staff interaction • Patient care delivery • Staffing • Medical record and logs in use
Patient Sample Selection • Ten percent sample with a minimum of 5 and maximum of 15. • Sample from ALL treatment modalities offered. • Selection made from information provided by the facility and general observations. • Cumulative lab reports, infection logs, hospitalization logs, vascular access information, pediatric patients, LTC facility patients, unstable patients are all used to select sampled patients.
Patient Interviews • Minimum of 5 patients • Can be same as sampled or different. • Done in treatment area, waiting room, in private or by phone • STAR has a structured guide or may use “custom” questions
Sample of Interview Questions • How do you participate in your plan of care? (V541, V 556) • How does your dialyzer look when your treatment is finished? V547) • Do you have a problem with your blood pressure? • Is your weight goal generally achieved? • Have you had any problems while on dialysis such as itching, chills, fever? • What happened? How did staff respond?
Medical Record Review~How Will Surveyors Know the POC Is Implemented? • Physician’s orders • Laboratory values • IDT progress notes • POC changes and updates • Dialysis flow sheets
Medical Record Review • FORMAT-electronic, manual or combination • CONTENT- Consents, Medical Exam, Histories, Progress notes, Labs, Treatment orders, Dialysis treatment records, Patient educations, Patient Assessment, POC, Demographic Information, Anemia management records, plus information from other disciplines.
Treatment Orders • Peritoneal dialysis treatment orders contain the Number of Exchanges and Dialysate Concentration-Volume. • Hemodialysis treatment orders contain- Treatment duration and frequency, BFR (Blood Flow Rate), Dialyzer, Dialysate Rx and flow rate, Target weight, Heparin dosing and other medications.
Dialysis Treatment Records • PD- contain flowsheets can be electronic or manual and are reviewed at least every 2 months. • Hemodialysis-contain Pre-Treatment, During Treatment and After treatment information
Hemodialysis Pre-treatment RecordSurveyors Look For: • Water Treatment • Dialysis machine • Reprocessed dialyzer checks • Dialysis orders • Patient information-demographic information
Machine Safety and Reprocessed Dialyzer Checks • Machine assessment-conductivity machine____manual____ pH____machine ____manual Alarm test Air detector on UF system Positive Presence Test___ Negative Residual Test___ Dialyzer ID___ Machine ID_____
Treatment Orders-examples • Dialyzer____DFR____BFR____Tx Time___ Dialysate______K_____Ca_____Bicarb____ Sodium Modeling_________ UF Profiling____ Dialysate temp______
Pre-Treatment, Post-Treatment Information • Include B/P – sit____stand___ • Weight_____ EDW___Wt gain__ • Wt loss___Wt removed_____ • Time on___time off____ • Assessment of patients GI, Cardiac, Edema, Mental, Mobility, and Access
Hemodialysis Treatment Records • Surveyors review orders, tx records and observe treatments to ensure all orders are followed pre-treatment, during treatment, and post treatment. Review for intradialytic patient and machine monitoring, medication and treatments administered. Heparin or anticoagulation are reviewed and compared with orders, observations, and interview information.
Immunization Medical Record Documentation • V 506, V 126, and V 127 • Record of testing and immunizations • Documentation of immunity or acknowledgement of absence of immunity • Documentation of further action planned if required.
Medical Record Documentation for Access and Adequacy • If expected outcomes for dialysis access or adequacy are NOT achieved, there should be evidence of reassessment for that aspect of care. • If the patient is not achieving the expected targets, there should be documentation of the reason WHY and a change in plan • Adjust the plan and implement the changes.
Medical Record Documentation for Access and Adequacy • May be in IDT assessments • Plan of care • Implementation of the care plan may be on flowsheets, progress notes, physician orders, etc.
Medical Record Documentation for Anemia Management • IDT assessments • Plan of care with measurable goals and timelines • Implementation of care plan: flowsheets progress notes medication administration records physician orders…etc
Medical Record Documentation for Nutrition • IDT assessment • Plan of care with measurable goals and timelines • Implementation of care plan flowsheets progress notes medication administration records physician orders…etc
Medical Record Documentation for Psychosocial • V 730- Results of standardized survey of mental and physical assessment (chosen by social worker) • Plan for psychosocial interventions (counseling and referral) to achieve and sustain appropriate psychosocial status • Plan for other elements of care that may be influenced by psychosocial status • IDT assessment • POC with goals and timelines • Implementation documentation in flowsheets, progress notes…etc….
Types of Medical Record Review • Comprehensive-all components are reviewed • Focused-review based on the rationale for sampling. Review areas of concern from survey or other records MAT will be used for reviews-see example
Patient Assessment and Patient Plan of Care • CFR 494.80 Patient Assessment The IDT must provide each patient an individualized comprehensive assessment- V501 There are 14 assessment criteria- V502-515. Reassessment frequency criteria is defined at V515-520. Kelly gave examples of the IDT POC and its correlation with the PA.
Staffing –COP V 750 • 494.180 Governance-addresses the overall management of the facility. The GB must demonstrate: Responsibility for the operation of the facility: Fiscal management Staff Training and Coverage Medical Staff appointments and coverage QAPI
Survey Process -Staffing • V 757and V 758 require the GB to ensure adequate numbers of qualified personnel are present for the patient/staff ratio is appropriate and meets the needs of patients. The RN, social worker and dietitian members of the IDT are available to meet patient clinical needs.
Staffing Surveyors consider patient acuity and care needs of patients, staff experience and areas of expertise. Staffing assignments and schedules reviewed to determine if there is a pattern of sufficient staff coverage to ensure safe patient care.
Staffing review continued: • If the facility “shares”the social worker or dietitian with multiple clinics or requires professional staff to perform non-clinical tasks, it must NOT negatively impact the time available to provide clinical interventions require to achieve the goals identified in the patient’s POC. The facility CEO or administrator is RESPONSIBLE to assure professional support staff members have sufficient time available in the facility to meet the clinical needs of in-center and home dialysis patients.
Surveyor Interviews With Professional Staff • Interview Professional staff to determine their professional duties and number of non-clinical duties. • Determine if non-clinical duties or tacks negatively impact the time available to provide clinical interventions and implementation of the plan of care.
Positive Patient Outcome • The renal community, CMS, state agency, and Network all work together to improve patient outcomes.
Questions??? • Liza Ben Vaughn, RN Email- lbenvau@kdhe.state.ks.us 785-207-0203