Download
1 / 49
510 likes | 908 Views
ASSESSING THE RESPIRATORY SYSTEM. Outcomes. Identify pertinent respiratory history questions. Obtain a respiratory history. Perform a respiratory physical assessment. Document respiratory assessment findings. Identify actual/potential health problems stated as nursing diagnoses.

E N D
Outcomes • Identify pertinent respiratory history questions. • Obtain a respiratory history. • Perform a respiratory physical assessment. • Document respiratory assessment findings. • Identify actual/potential health problems stated as nursing diagnoses. • Differentiate between normal/abnormal findings.
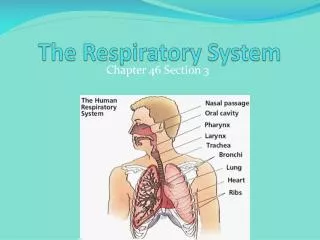
Anatomy Review Structures *Nasal cavity *Pharynx *Larynx * Trachea *Bronchi * Bronchioles *Alveolar ducts and sacs *Pleura
Functions Nasal cavity: Warms, humidifies, and filters air Pharynx: Passageway between nose and larynx, and mouth and esophagus Larynx: Passageway; contains voice box (Continued)
Functions Trachea: Airway between larynx and bronchi Bronchi: Airways with primary, secondary, and tertiary branches Bronchioles: Transitional airways; some gas exchange occurs here (Continued)
Functions Alveolar ducts and sacs: Functional units for gas exchange Pleura: Serous protective lining of the lungs; reduces friction and helps maintain negative pressure
Acid-Base Balance • It is the 1st system to respond to blood acidity • Responds by changing the depth & rate of respirations • CO2 is converted to bicarbonate (carbonic acid) • In metabolic acidosis (excess acid retention), the rate & depth INCREASES to “blow off” excess CO2 (reducing the amount available to make carbonic acid) = thus decreasing hydrogen ions and increasing pH
Acid-Base Balance • In metabolic alkalosis (excess of base), the rate and depth will decrease to conserve carbon dioxide. • Hyperventilation can result in respiratory alkalosis • Hypoventilation can result in respiratory acidosis
Relationship to Other Systems *Integumentary • Protects structures of UR tract • Nasal hair filters air *Digestive • Abdominal muscles aid with respirations • GI tract provides nutrients to Respiratory System
Relationship to Other Systems *Cardiovascular • Transports O2 and CO2 between lungs and peripheral tissue • Activation of angiotensin by lungs important in BP regulation • Peripheral chemoreceptors in aortic arch & carotid arteries respond to O2, CO2, and H+ ion concentrations
Relationship to Other Systems *Musculoskeletal • Diaphragm, chest & abdominal muscles needed for breathing • Accessory muscles used when O2 demands increased (eg: strenuous exercising) • Ribs provide protective covering for lungs
Relationship to Other Systems *Endocrine • Converting enzymes in lung convert angiotensin I to angiotensin II. • Epinephrine and norepinephrine increase respiratory rate and dilate airways *Neurological • Medulla is respiratory center • Chemoreceptors respond to changes in CO2, O2, and H+ by affecting rate & depth of respirations
Relationship to Other Systems *Lymphatic • Alveolar macrophages trap microorganisms & other foreign substances • Foreign material removed by cilia or lymph • Tonsils & adenoids protect upper airways from infection but also may become enlarged & obstructive *Reproductive • Sexual activity increases oxygen demands • Pregnancy affects oxygen demands & breathing
Relationship to Other Systems *Urinary • GU system works with respiratory system to eliminate wastes and maintain acid base balance (pg 395)
DevelopmentalVariations • Infants • Nose breathers (bronchovesicular) • Respirations are primarily abdominal (shifts to intercostal after age 2) • Respiratory rhythm is irreg. (apnea should never exceed 15 seconds)
DevelopmentalVariations • Pregnant Women • Increases in tidal volume and respiratory rate allow for a 20 % increase in O2 demand • Later in pregnancy the diaphragm rises and the costal angle widens to accommodate the enlarging uterus
DevelopmentalVariations • Older adults • Alveoli tend to fibrose with age (decreased surface area for gas exchange) • Lung capacity decreases due to muscle weakness & less elasticity • More “dead” space, trapped air, less vital capacity • Often the thoracic spine curve (kyphosis) may give appearance of a barrel chest (this does not usually result in dysfunction)
Cultural Variations • African Americans • Higher risk of respiratory disease due to living in urban areas • Asians • Smaller chests than Euro/African • Appalachians/Irish • Higher risk for black lung, emphysema, TB • Native Americans • Reservated NA more at risk related to close living quarters
Katie Kane, 38-year-old, married, accountant, mother of three children scheduled for laparoscopic cholecystectomy with general anesthesia preop workup Case Study
HistoryWhat can the history tell you about the respiratory system? • Biographical data • Current health status • Past health history • Family history • Review of systems • Psychosocial history
SymptomsWhat symptoms would signal a respiratory problem? • Cough • Dyspnea • Chest pain • Edema • Fatigue
Pertinent History Findings • + frequent URI as a child; exposed to second-hand smoke • + family history of smoking and lung cancer • Overweight (Continued)
Pertinent History Findings • Smokes 1 pack/day/10 years • + productive (whitish-gray mucous) morning cough past 5 years • + family support for post-operative care
Physical Assessment Anatomical landmarks: anterior, posterior, and lateral approach; work apex to base; compare side to side Approach: all 4 techniques Position: sitting Tools: stethoscope General survey and head-to-toe scan
Inspection • Respiratory rate, rhythm, pattern • Size, shape, and symmetry of chest • AP:lateral ratio (normal 1:2) • Costal angle (normal < 90 degrees) (Continued)
Inspection • Muscles for breathing • Condition of skin • Spinal deformities • Abnormal findings
Palpation • Tracheal position • Chest tenderness • Chest excursion (expansion; 3-6cm) • Tactile fremitus (vibration – “99”) • Crepitus (air in subcutaneous tissue) • Abnormal findings
Palpation Light: non-tender, no deformities or crepitus Excursion: symetrical without lag Tactile Fremitus: equal bilaterally and diminished midthorax
Percussion • Percuss chest • Diaphragmatic excursion • Abnormal findings
Percussion Dullness: seen with exudate, fluid, tumors, pneumonia, pulmonary edema, pleural effusion
Diaphragmatic Excursion: measures symmetrical expansion of the diaphragm through percussion & measurement • It take great skill to learn this • Decreased Diaphragmatic Excursion can be a sign of paralyzed diaphragm, atelectasis, COPD with overinflated lungs • Normal is 3-6cm
Auscultation Breath sounds: • Normal • Abnormal
Pertinent Physical Findings • Respirations 16/min. • Symmetrical excursion • Lung fields resonant; diaphragmatic excursion 4 cm • Nicotine stained fingers • Expiratory wheezes clear with coughing
Nursing Diagnosis What actual or potential problems can you identify for Mrs. Kane?
Nursing Diagnosis • Infection, risk for • Activity intolerance • Breathing pattern, ineffective • Pain, self-management • Anxiety • Potential complication: atelectasis • Scheduled for cholecystectomy with general anesthesia, smoking history
Auscultation Breath sounds: • Vesicular • Bronchovesicular • Bronchial (Continued)
Auscultation Adventitious breath sounds: • Rales/Crackles • Rhonchi/Wheezes • Friction Rub • Stridor • Grunting (Continued)
Auscultation Abnormal voice sounds: • Bronchophony (Abnormal Clarity) • Egophony (Voice of the goat: “eee”= “ay”) • Whispered Pectoriloquy (“1-2-3”)