Download
1 / 10
100 likes | 109 Views
A compile of the 1918 outbreak and the potential protagonists and what was known at the time

E N D
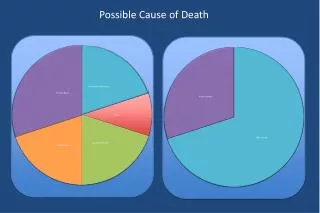
Predominant Role of Bacterial Pneumonia as a Cause of Death in Pandemic Influenza: Implications for Pandemic Influenza Preparedness J Infect Dis. October 1, 2008; An important question related to pandemic preparedness remains unanswered: what killed people during the 1918–1919 pandemic and subsequent influenza pandemics? In the present study, we have examined recut tissue specimens obtained during autopsy from 58 influenza victims in 1918–1919, and have reviewed epidemiologic, pathologic, and microbiologic data from published reports for 8398 post-mortem examinations bearing on this question. We have also reviewed relevant information, accumulated over 9decades, related to the circulation of descendants of the 1918 virus. With the recent reconstruction of the 1918 pandemic influenza virus, investigators have begun to examine why it was so highly fatal [6,7]. Based on contemporary and modern evidence, we conclude here that influenza A virus infection in conjunction with bacterial infection led to most of the deaths during the 1918–1919pandemic. Background epidemiologic data on influenza mortality rates in 1918–1919 Although death certificates listing cardiac and other chronic causes of death increased in number during the time frame of the 1918–1919 pandemic [18], for all age groups death was predominantly associated with pneumonia and related pulmonary complications [13,14, 18-20]. Histologic examination of lung tissue from 1918 victims The examination of recut lung tissue sections from 1918–1919 influenza case material revealed, in virtually all cases, compelling histologic evidence of severe acute bacterial pneumonia, either as the predominant pathologyor in conjunction with underlying pathologic features now believed to be associated with influenza virus infection [10,24] The majority of the cases examined demonstrated asynchronous histopathological changes, in which the various stages of development of the infectious process, from early bronchiolar changes to severe bacterial parenchymal destruction, were noted in focal areas. Published pathologic and/or bacteriologic findings from the 1918–1919 influenza pandemic Although the cause of influenza was disputed in 1918, there was almost universal agreement among experts [e.g., 20,27–33] that deaths were virtually never caused by the unidentified etiologic agent itself, but resulted directly from severe secondary pneumoniacaused by well-known bacterial “pneumopathogens”that colonized the upper respiratory tract(predominantly pneumococci, streptococci, and staphylococci). Without this secondary bacterial pneumonia, experts generally believed that most patients would have recovered [20].
Repair, represented by early epithelial regeneration, capillary repair, and occasionally by fibrosis, was commonly seen in tissues sections from even the most fulminant fatal cases [20,27,32]. Among the ≥60% of individuals who survived such severe pneumonia, severe chronic pulmonary damage was apparently uncommon [37,38]. Many of the series were methodologically rigorous: in one study of approximately 9000 subjects who were followed from clinical presentation with influenzato resolution or autopsy [40], researchers obtained, with sterile technique, cultures of either pneumococcior streptococcifrom 164 of 167 lung tissue samples. There were 89 pure cultures of pneumococci; 19 cultures from which only streptococci were recovered; 34 that yielded mixturesof pneumococci and/or streptococci; 22 that yielded a mixture of pneumococci, streptococci, and other organisms (prominently pneumococciand nonhemolytic streptococci); It is noteworthy that pneumococcal typing antisera were unavailable in 11 of these 14 studies, and that many of the cultured “other” bacteria were reported as “gram-positive diplococci,” “streptococci,” or “diplostreptococci” (data not shown), consistent with the possibility that in this early era of bacterial typing, some of the unidentified organisms in the culture may have been pneumopathogens The virusesthat caused the 1957 and 1968 pandemics were descendants of the 1918 virusin which 3 (the 1957 virus) or 2 (the 1968 virus) new avian gene segments had been acquired by reassortment[21]. Although lower pathogenicity resulted in far fewer deaths, hence fewer autopsies, most 1957–1958deaths were attributable to secondary bacterial pneumonia, as had been the case in 1918. Staphylococcus aureus, a relatively minor cause of the 1918 fatalities, was predominant in the culture results from1957–1958 [21,57-61], and negative lung tissue cultures were more common, possibly as a result of the widespread administration of antibiotics [57,58,61]. Thepneumonia deaths during the influenza pandemic in 1918proved so highly similar, pathologically, to the then-recent pneumonia deaths from the measles epidemics that noted experts considered them to be the result of one newly emerging disease:epidemic bacterial pneumoniaprecipitated by prevalent respiratory tract agents [20, 33,63]. In 1935, Brightman studied combined human influenza and streptococcal infectionin a ferretintranasalinoculationmodel. Even though neither agent was pathogenic when administered alone, they were highly fatal in combination[68]. In rhesus monkeys, human influenza viruses givenintranasally were not pathogenic, butcould be made so by nasopharyngeal instillation of otherwise nonpathogenic bacteria[69].
During the 1940s, additional studies in ferrets, mice, and ratsestablished that the influenza virus in combination with any of several pneumopathic bacteria acted synergisticallyto produce either a higher incidence of disease, a higher death rate, or a shortened time to death [70-73]; As reviewed recently by McCullers [75], a body of experimental research during the last 3 decades has identified possible mechanisms by which co-infection with the influenza virus and bacteria might affect pathogenicity…such as virus-induced desensitization to bacterial Toll-like receptor ligands [79] and interleukin 10–induced susceptibility to pneumococci and possibly staphylococci [76]; We believe that the weight of 90 years of evidence (table 3), including the exceptional but largely forgotten work of an earlier generation of pathologists, indicates that the vast majority of pulmonary deaths from pandemic influenza viruses have resulted from poorly understood interactions between the infecting virus and secondary infections due to bacteria that colonize the upper respiratory tract. The extraordinary severity of the 1918 pandemic remains unexplained. That the causes of death included so many different bacteria, alone or in complex combinations, argues against specific virulent bacterial clones. The 1918 pandemic and subsequent pandemics differed with respect to the spectrum and extent of secondary bacterial pneumonia(e.g., the switch in prevalence during the antibiotic erato predominantly staphylococcal secondary pneumonia, as opposed to streptococcal, pneumococcal, and mixed secondary pneumonia; and the greatly decreased involvement of Bacillus[Hemophilus] influenzae), suggesting that additional factors affectthe level of influenza morbidity and mortality The aging population in the United States, the increasing number of persons living in nursing home facilities, and the number of persons who are immunosuppressed or affected by cardiac disease, renal disease, and/or diabetes mellitus all represent potential factors that might change the profile of morbidity and mortality during a future pandemic. For example, elderly persons in nursing homes are at risk for pneumoniacaused by enteric organisms and sometimes by drug-resistant nosocomial organisms. The spread of bacteria such as methicillin-resistant Staphylococcus aureus(MRSA) and highly pathogenic clones of Streptococcus pyogenes pose more general risks[86]. If the next pandemic is caused by a human-adapted virus similar to those recognized since 1918, we believe the infection is likely to behave as it has in past pandemics, precipitating severe disease associated with prevalent colonizing bacteria.
1 Enzyme activity measurement showed that L-ascorbic acid (vitamin C (Vc)) competitively inhibits thehyaluronan degradation by Streptococcus pneumoniaehyaluronate lyase. The high concentration of Vcin human tissues probably provides a low level of natural resistance to the pneumococcal invasion. This is the first time that Vc the direct inhibition on the bacterial “spreading factor” was reported, and Vc is also the first chemical that has been shown experimentally to have an inhibitory effect on bacterial hyaluronate lyase. Vc is a multifunctional molecule in tissues. It usually acts as an antioxidant (3), free radical scavenger (4), neuroprotectant, and neuromodulator (5). It also plays an important physiological function in activating peptide hormones (2) and regulating cell division and growth (6). Streptococcus pneumoniae is a Gram-positive bacterial pathogen that causes pneumonia, bacteremia, meningitis, sinusitis, and otitis media in humans worldwide, especially in neonates and children, and often leads to significant rates of mortality and morbidity. It secretes hyaluronate lyase to catalyse the degradation of hyaluronan (HA), one of the main components of connective tissues in animals, to expose tissue cells to bacterial toxins. The inhibition of hyaluronate lyase is expected to reduce the spreading of this pathogen in the most early stages of pneumococcal invasion. The action mechanism of hyaluronan degradation by Streptococcus pneumoniae hyaluronate Lyase [SpnHL], which was revealed recently, provides a unique opportunity to targethyaluronate lyase in the prevention of the pneumococcal invasion. Conclusions and General Implications Vcmay compress or retardbacterial invasion by directly inhibiting the bacterial spreading factor, such as hyaluronate lyase, through binding to the enzyme active site and competing with the binding of thehyaluronan substrate. All seven protein interface residues interacting with Vc are strictly conserved among all known bacterial hyaluronate lyases (8). The studies on the SpnHLzVc interface are thus significantly relevant to all thesebacterial hyaluronate lyases. The results shown may be applicable to Streptococcus agalactiae hyaluronate lyase, which means that Vc might also provide the host with the ability to resist the S. agalactiae invasion to a certain extent. This is the first time that the direct action of Vc on a bacterial spreading factor has been observed. 1 2001, Vitamin C Inhibits the Enzymatic Activity of Streptococcus pneumoniae Hyaluronate Lyase*
Hyaluronidases are enzymes that degrade hyaluronan, an important component of the extracellular matrix. The mammalian hyaluronidasesare considered to be involved in many (patho)physiological processes like fertilization, tumor growth, and metastasis. Bacterial hyaluronidases, also termed hyaluronate lyases, contribute to the spreading of microorganisms in tissues. Here we show that L-ascorbic acid 6-hexadecanoate (Vcpal) is a potent inhibitor of bothstreptococcal and bovine testicular hyaluronidase (BTH). To date, Vcpalhas proved to be one of the most potent inhibitors of hyaluronidase. In our normalized assays with equiactive concentrations the bacterial enzymes were weakly inhibited by Vc with IC50 values of 6 mMfor SagHLand 32 mMfor SpnHL, respectively, whereas the bovine enzyme was not affected up to 100 mM. Therefore, Vc proved to be a weak but selective inhibitor of streptococcal hyaluronate lyases. Under physiological conditions Vc is suggested to trigger a natural, low level defense mechanism in the human organism against pneumococcal invasion. In agreement with the inhibitory effects that have been observed for various fatty acids on S. dysgalactiaehyaluronidase (26), hexadecanoic acid (L-Ascorbic Acid Hexadecanoate) showed an inhibition of the activity ofSagHLby 80% at maximal test concentration of 295 uM, whereas Vcpal strongly inhibitedSagHLwith an IC50 of 4 uM(Fig. 2). Equiactive concentrations of SpnHL and bovine testicular hyaluronidase revealed IC50 values of 100 and 56 uM, respectively. Thus, Vcpal is up to 1500 times more active than Vcand proved to be among the most potent inhibitors ofbacterial and bovine hyaluronidasesdescribed to date 2 2004, L-Ascorbic Acid 6-Hexadecanoate, a Potent Hyaluronidase Inhibitor
Abstract Supraphysiologicalconcentrations of oxygen (hyperoxia) can compromise host defense and increase susceptibility to bacterial infections, causing ventilator-associated pneumonia. The phagocytic activity of macrophagesis impaired by hyperoxia-induced increases in the levels of reactive oxygen species (ROS) and extracellular high mobility group box protein B1 (HMGB1). The aim of this study was to determine whether AA could attenuate hyperoxia-compromised host defenceand improve macrophage functions against bacterial infections. C57BL/6 male mice were exposed to hyperoxia(>98% O2, 48 h), followed by intratracheal inoculation with Pseudomonas aeruginosa, and simultaneous intraperitoneal administration of AA. AA (50mg/kg) significantly improved bacterial clearance in the lungsand airways, and significantly reduced HMGB1 accumulation in the airways Clinical Relevance Patients receiving oxygen therapy are highly susceptible to pulmonary infections, which may lead to ventilator-associated pneumonia(VAP). Data in this study suggest that ascorbic acid (AA) levels can be significantly reduced in patients receiving oxygen therapy, and AA supplementation can prevent or attenuatethe development of VAP in these patients. Thus, our findings demonstrate that boosting the host defence with a simple and inexpensive antioxidant, ascorbate, may help to reduce mortality and morbidity in patients receiving oxygen support. Prolonged exposure to hyperoxia can compromise the host defense against bacterial infections by impairingthe efficacy of alveolar macrophages to migrate, phagocytose, kill, and clear bacteria(7, 13–18). Hyperoxia-induced deleterious effects are mainly attributable to an increase in the levels of reactive oxygen species (ROS), resulting in oxidative stress, which ultimately surmount the antioxidant defense mechanisms(19, 20). ROS can cause lipid peroxidation, protein, and DNA oxidation, and alter signal transduction pathways, leading to cell damage(21–25). Hyperoxia-exposed cells overexpressing antioxidant enzyme, manganese superoxide dismutase, exhibit reduced bacterial adherence, increased phagocytic activity (26, 27), and attenuated ROS-induced damage (28). These aforementioned findings suggest that antioxidantsmay be useful in attenuating ROS-induced cellular damage and impairment of macrophage functions. 3 2016, Ascorbic Acid Attenuates Hyperoxia-Compromised Host Defence against Pulmonary Bacterial Infection
Ascorbic acid (AA), an essential nutrient, is a well known reductant and scavenger of intracellularROS(29–32). AA can donate two electrons that are lost sequentially, and is considered to be an efficacious antioxidant, as it reduces a reactive free radical with the formation of a less reactive compound (30, 33, 34). In mice (Animal Studies: C57BL/6 mice (male, 8–12 week old) exposed to hyperoxia, elevated levels of airway HMGB1 are associated with an increase in both the lung bacterial burden and lung damage. Neutralizingor inhibiting HMGB1by monoclonal antibodiesor compounds, significantly decreases lung injury and hyperoxia-compromised bacterial clearance (7, 38). These results indicate that AA improvesbacterial clearance and acute lung injury, whichresults in an increase in survival in this mouse model of VAP. These results suggest that AA can enhanceinnate immunity againstbacterial infections by improving macrophage phagocytic activity under hyperoxic conditions. AA showed a concentration-dependent decrease in ORP, which was significantly less at 1,000 μM, compared with macrophagesexposed to hyperoxia in the absence of AA. These results suggest that AA enhancesmacrophage functions by bluntinghyperoxia-induced oxidative stress. Immune cells, especially macrophages, maintain very high concentrations of AA compared with plasma (40). To determine if exposure to hyperoxia altersAA levels in macrophages, the intracellular concentrations of AA were measured. Because AAwas undetectable in cultured RAW 264.7 cells (data not shown), RAW cells were incubated with 1,000 μM AA for 1 hour before hyperoxia exposure. Exposure to hyperoxia significantly reduced the intracellular AA levels compared with control RAW cells exposed to room air. These data indicate that intracellular AA levels in macrophages are rapidly exhausted upon hyperoxia exposure. We further investigated whether continuous AA (10–1,000 μM) supplementation for 24 hours with simultaneousexposureof RAW cells to hyperoxia can maintainintracellular AA levels. Data presented in Figure 4B show that RAW cells with supplementation of 1,000 μM AA had similar intracellular AA levels uponexposure to hyperoxia as that of room air–exposed cells. However, intracellular AA levels were significantly lower in hyperoxia-exposed cells when RAW cells were supplemented with 10 or 100 μM AAas compared with the room air control groups. These results suggest that a continuous supply with appropriate concentrations of AA mitigateshyperoxia-induced decrease in intracellularAAlevelsand maintains the intracellular antioxidant capacity. (Note: Many studies suggest using much higher doses and for longer periods in acute and chronic disease)
The translocation of HMGB1 from the nucleusto the cytoplasm is a critical stepin the extracellular secretion of HMGB1 (42, 43). Therefore, we determined the effect of AA onthenucleocytoplasmictranslocation of HMGB1 in hyperoxic macrophages. These results indicate that AA significantly reducesthe hyperoxia-elevatedHMGB1 accumulation in the extracellular milieu by inhibitingits translocationfrom the nucleustothe cytoplasm. NF-kB activation plays a critical role in mediating the release of HMGB1 from cultured macrophages under stress stimuli, including exposure to hyperoxia(17, 38, 44). NF-kBactivation was assessed by immunostaining the p65 subunit of NF-kB, as described in the published studies. Upon hyperoxic exposure, NF-kBtranslocates into the nucleus,as indicated by a profound nuclear staining. However, macrophagesexposed to hyperoxia and incubated with AA at 1, 100, and 1,000 μM had significantly reduced nuclear staining compared with cells exposed to hyperoxia alone. These results suggest that AA inhibitsHMGB1 release, at least in part, by preventinghyperoxia-induced NF-kBactivation. Discussion The results of this study indicate that AA protectsagainst hyperoxia-induced lung injury and enhances innate immunity against pulmonary PA infection in a mouse model of VAP. In addition, AA can effectively restorehyperoxia-compromisedphagocytic function of cultured macrophages. AA-increasedmacrophage phagocytic function was associated with a decrease inhyperoxia-induced: (1) elevation in intracellular oxidative stress; and (2) accumulation of extracellular HMGB1. The AA-mediated decrease in the extracellularaccumulation of HMGB1was associated with inhibition of thetranslocationofnuclear HMGB1 to the cytoplasm, was associated with attenuatedNF-kB activation. Hyperoxia-induced lung permeability, a marker of tissue injury, can also be reduced by AA(Figure 1C). This increase in host immunity was associated with an improved survival of these animals. Interestingly, AA did not significantly increase bacterial clearance and lung injury under normoxic (healthy) conditions. Similarly, AA(100 mg/kg/12 h) does not significantly increase the clearance of Streptococcus pneumoniae in normoxic, healthy mice (46). A similar protective effect of AA (50 or 200 mg/kg/24 h) against organ failure and tissue injury has also been observed in patients with severe sepsis (49). These findings suggest that the protective effect of AA is specific to pathological conditions with AA deficiency. AA has also been shown to decrease the levels of the hydrogen peroxide–inducedROS (51). Similar to these observations in macrophages, AA has also been shown to improvephagocytic functions of monocytes and neutrophils in humans(53, 54) and murineperitonealmacrophages(55, 56). These results demonstratethat AAcan effectively maintainthe phagocytic functions of macrophages under oxidative stress.