Download
1 / 22
220 likes | 224 Views
AstraZeneca, Oxford University and AZD122 (ChAd0X1) Adenovirus Ad26 vector-based vaccine now called as a commercial product 'Vaxzevria'<br>

E N D
AstraZeneca, Oxford University and AZD122 (ChAd0X1) Adenovirus Ad26 vector-based vaccine
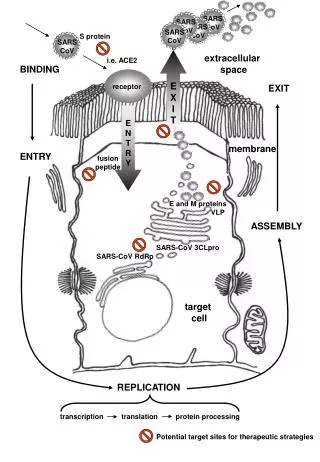
Study: Single-shot Ad26 vaccine protects against SARS-CoV-2in rhesus macaques Published online: 30 July 2020 - Nature The optimal Ad26 vector-based vaccine for SARS-CoV-2, termed Ad26.COV2.S, is currently being evaluated in clinical trials. Fifty-two rhesus macaques were immunized with Ad26 vectors encoding S variants or sham control, without adjuvantat week 0. and were challenged with SARS-CoV-2 by the intranasal and intratrachealroutes (of those,S.dTM.PP (N=6),S.PP (N=6), which have Furin cleavage site mutations Median Nab (Neutralising antibodies) titers in the Ad26-S.PP vaccinatedmacaques were 4-fold higher than median Nab titers in previously reported cohorts of 9 convalescent macaques [9] and 27 convalescent humans following recovery from SARS-CoV-2 infection [10] The Ad26-S.PP vaccine also induced detectable S-specific IgG and IgA responses in bronchoalveolarlavage (BAL) Analysis of a cohort of 10 similarly immunized animals demonstrated that a single immunization of 1011vpAd26-S.PP elicited consistent IFN-γ ELISPOT responses but minimal to no IL-4ELISPOT responses, suggesting induction of Th1-biased responses. At week 6, all animals were challenged with 1.0x105 TCID50 (Tissue Culture Infectious Dose) SARS-CoV-2 (which was derived from USA-WA1/2020(NR-52281; BEI Resources [9]) by the intranasal (IN) and intratracheal (IT) routes. Ad26 vectors were constructed with seven variants of the SARS-CoV-2 spike (S) protein sequence (Wuhan/WIV04/2019; GenbankMN996528.1). The S.PP immunogencontains the wild-type leader sequence, the full-length membrane-bound S, mutation of the furin cleavage site, and two proline stabilizing mutations[15].
Whereas inactivated virus vaccines and nucleic acid vaccines typically require two or more immunizations, certain adenovirus vectorscan induce robust and durable NAb responses after a single immunization [22–24]. However, we would expect that a two-dose vaccine with Ad26-S.PP would be more immunogenic... both single-doseand two-dose regimens of the Ad26-S.PP vaccine should be evaluated in clinical trials These data suggest that serum NAb titers may be a potential biomarker for vaccine protection, although thiswill need to be confirmedin additionalSARS-CoV-2 vaccine efficacy studies in both nonhuman primates and humans. The roleof T cell responsesin vaccine protection remains to be determined. Our studies also were not specifically designed to assess safety or the possibility of vaccine-associated enhanced respiratory disease or antibody-dependent enhancement (ADE) of infection[29] However, it is worth noting that the Ad26-S.PP vaccine elicited Th1-biasedrather than Th2-biased T cell responses, and animals with sub-protective NAb titers did not demonstrate enhanced viral replication or clinical disease It is likely that protection in both the upper and lower respiratory tracts will be required to prevent transmission and disease in humans. The identification of a Nab correlate of protection should prove useful in the clinical development of SARS-CoV-2 vaccines. The optimal Ad26-S.PP vaccine from this study, termed Ad26.COV2.S, is currently being evaluated in clinical trials. Western blot - 24 well plates were seeded with MRC-5 cells(1.25x105 cells/well), and after overnight growth they were transduced with Ad26 vectors encoding SARS-CoV-2 Spike transgenes. CR3046 is a human monoclonal antibody directed against SARS-CoV Spikeand binds to the Spike S2 domainand also cross-reacts with SARS-CoV-2 Spike S2 (unpublished data). Plaque-forming unit (PFU) assay: For plaque assays, confluent monolayers of Vero E6 cellswere prepared in 6-well plates.
Pseudovirus neutralization assay - The SARS-CoV-2 pseudoviruses expressing a luciferase reporter genewere generated in an approach similar to as described previously [9,10,16]. Briefly, the packaging construct psPAX2 (AIDS Resource and Reagent Program), luciferase reporter plasmid pLenti-CMV Puro-Luc (Addgene), and spike protein expressing pcDNA3.1-SARS-CoV-2 SΔCT were co-transfected into HEK293T cells with calcium phosphate. The supernatants containing the pseudotype viruseswere collected 48 hpost-transfection; To determine the neutralization activity of the antisera from vaccinated animals, HEK293T-hACE2 cellswere seededin 96-well tissue culture plates at a density of 1.75 x 104 cells/well overnight. Live virus neutralization assay - A full-length SARS-CoV-2 virus based on the Seattle Washington isolate was designed to express nanoluciferase(nLuc) and GFP and was recovered via reverse genetics and described previously [17,18]. luciferase activity was measured via Nano-Glo Luciferase Assay System (Promega) IFN-γ enzyme-linked immunospot (ELISPOT) assay:ELISPOT plates were coated with mouse anti-human IFN-γ monoclonal antibody from BD Pharmingen at a concentration of 5 μg/well overnight at 4 °C. The plates were washed with coulter buffer and incubated for 2 h with Rabbit polyclonal anti-human IFN-γ Biotin from U-Cytech(1 μg/mL).
COVID-19 (SARS-Cov-2) FRONT RUNNERS University of Oxford, AstraZenecaand partners– AZD1222 (formerly ChadOx1 nCoV-19) Phase III D8110C00001 trial (NCT04516746) – Adenovirus Type 26 (Ad26) 1AstraZenecaacknowledged September 8 that it paused (but has not disclosed specifics on the adverse reaction and when it took place) the up-to-30,000 patient Phase III trial of AZD1222to investigate a “potentially unexplained illness” involving a participant from the U.K. UK health secretary Matt Hancock said “30 million doses already contracted with AstraZeneca” On September 7, Australia’s federal government has reached agreement with Melbourne-basedCSL to manufacture a total 84.8 million doses of AZD1222 and V451, a vaccine developed by CSLwith the University of Queensland AlbanyMolecular Research, Inc. (AMRI) to provide sterile fill/finish of AZD1222through 2021 at AMRI’sdrug product manufacturing facility in Albuquerque, NM, under a supply agreement announced September 3 by AMRI September 1, AstraZenecaagreed to pay Oxford Biomedicaa £15 million ($20.1 million) upfront capacity reservation fee under an 18-month supply agreement announced by Oxford Biomedica (Oxbox commercial manufacturing center in Oxford, U.K), part of a three-year Master Supply and Development Agreement with AstraZeneca for large-scale commercial manufacture of AZD1222. Oxford Biomedica’s partnership established in June with the UK’s Vaccine Manufacturing Innovation Centre (VMIC). AZD1222has been developed by the University’s Jenner Institute. U.K. Health Secretary Matt Hancock pledged £20 million ($25 million) in government funding to support development of the vaccine. 1 https://www.genengnews.com/covid-19-candidates/university-of-oxford-and-partners/
“Unlike CanSino, Modernaand Pfizer, AstraZenecaand Oxford University only tested one high-dosage formulationof the vaccine, providing less data on the optimal relation of antibody response induction to acceptable side effects,” PhilippRosenbaum, PhD, Senior Infectious Diseases Analyst and Breen, PhD, Director of Infectious Diseases at GlobalData, stated. “In the context of a pandemic wave where a single higher, but more reactogenic, dose might be more likely to rapidly induce protective immunity, the use of prophylactic paracetamol appears to increase tolerability and would reduce confusion with COVID-19 symptoms that might be caused by short-lived vaccine-related symptoms without compromising immunogenicity,” the researchers explained 1 Another £22.5 million is to fund Phase II testing of a coronavirus vaccine in development by Imperial College London, which is projected to start human testing in June. The Imperial College London funding will also be used to help prepare for Phase III studies. “We will throw everything we’ve got at developing a vaccine,” Hancock added. “The U.K. is at the forefront of the global effort … and for all of the efforts around the world, two of the leading vaccine developments are taking place here at home, at Oxford and Imperial.” The start of human testing in the U.K. coincides with Germany’s regulator, the Paul-Ehrlich-Institut, giving GermanbiotechBioNTechand partner Pfizer the green light (under global “Lightspeed” COVID-19 vaccine development program) to start the first coronavirus vaccine clinical trial in the country. The Phase I/II study will evaluate the BNT162 vaccine program in 200 healthy volunteers aged 18–55 years. Each candidate represents a different mRNA format and target antigen. Two of the fourvaccinecandidatesare nucleoside modified mRNA (modRNA) vaccines, a third is a uridine containing mRNA(uRNA), and the fourthvaccine candidate utilizes self-amplifying mRNA (saRNA). Each mRNA format is combined with a lipid nanoparticle (LNP) formulation. 1 https://www.genengnews.com/news/uk-starts-oxford-coronavirus-vaccine-trial-as-germany-green-lights-clinical-trial-for-biontech-and-pfizer/
The team started work on designing a coronavirus vaccine on January 10, 2020. Their vaccine candidate is based on a non-replicating chimpanzee adenovirus vector, ChAdOx1, which was originally developed at the Jenner Institute. Engineered to encode the SARS-CoV-2 spike protein, the ChAdOx1 nCoV-19 construct is designed to trigger production of the viral protein which then primes the immune system to recognizeSARS-CoV-2 infection. The Phase I ChAdOx1 nCoV-19 trial will be carried out through a collaboration between the Oxford Vaccine Group’s clinical teams and the University’s Jenner Institute, and include 510 volunteers aged 18–55 years. Imperial College London’s self-amplifying RNA vaccine, developed by a team led by Robin Shattock, PhD, at the department of infectious diseases, is designed to trigger muscle cells to produce the SARS-Co-2 spike protein that will stimulate the immune system to generate neutralizing antibodies against the virus. Tests in animals have been underway since February, and clinical trials could start in the summer, the team projects.
Study: Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine againstSARS-CoV-2: a preliminary report ofaphase I/II, single-blind, randomised controlled trial – 1090 Healthy adults aged 18–55 years - Published Online July20, 2020(ClinicalTrials.gov Identifier: NCT04324606) Funding UK Research and Innovation, Coalition for Epidemic Preparedness Innovations, National Institute for Health Research (NIHR), NIHR Oxford Biomedical Research Centre, Thames Valley and South Midland’s NIHR Clinical Research Network, and the German Center for Infection Research (DZIF), Partner site Giesen-Marburg-Langen Methods We did a phase 1/2, single-blind, randomised controlled trial in five trial sites in the UK of a chimpanzee adenovirus-vectored vaccine(ChAdOx1nCoV-19 (n=543))expressing the SARS-CoV-2 spike protein as a single intramuscular injectioncompared with a meningococcal conjugate vaccine(MenACWY) as control. 2 of 5 sites (Oxford and Southampton) a protocol amendment (amendment date May 6, 2020) allowed prophylactic paracetamol to be administered before vaccination. Safety was assessed over 28 days after vaccination. Here, we report the preliminary findings on safety, reactogenicity, and cellularand humoral immune responses. The study is on-going, and was registered at ISRCTN, 15281137, and ClinicalTrials.gov, NCT04324606 Local and systemic reactions were more common in the ChAdOx1 nCoV-19 group and many were reduced by use of prophylactic paracetamol (1 g of paracetamol every 6 h for 24 h to reduce vaccine-associated reactions)., including pain (injection site pain, tenderness, warmth, redness, swelling, induration, and itch), feeling feverish, chills, muscle ache, headache, fatigue, nauseaand malaise In the ChAdOx1 nCoV-19 group, spike-specific T-cell responses peaked on day 14 Added value of this study ChAdOx1 nCoV-19 has previously been reported to be immunogenic and protective against pneumoniain a rhesus macaque challenge model. We report the results of the first clinical study of ChAdOx1 nCoV-19 (AZD1222). The vaccinewas safe and tolerated, with reduced reactogenicity when paracetamol was used prophylactically for the first 24 h after vaccination.
There are currently more than 137 candidates undergoing pre-clinical development and 23 in early clinical development, according to WHO[2]. Implications of all the available evidence A vaccine against SARS-CoV-2 could be used to prevent infection, disease, and death in the global population, with high-riskpopulationssuch as hospital workersand older adults(eg, ≥65 years of age) prioritised to receive vaccination. Adenoviral vectors have previouslybeen combined with DNA and poxviral vectorsto attempt to improve immunogenicity, with adenovirusor modified vaccinia virus Ankara prime-boost regimens showing enhancement of both cellularand humoral immunity. We have previously shown (Clinical trial identifier: NCT04170829 ) that a single dose of ChAdOx1 MERS, a chimpanzee adenovirus vectored vaccinethat encodes the spike protein of Middle East respiratory syndrome coronavirus (MERS-CoV), protected non-human primates against MERS-CoV-induced disease [7] and data from a phase 1 clinical trial showed that ChAdOx1 MERS was safe and well tolerated at all three doses tested. In addition, the highest dose elicited both humoral and cellularresponses against MERS-CoVin all vaccineswithin 1 month of vaccination. The ChAdOx1 nCoV-19 vaccine (AZD1222) consists of the replication-deficient simian adenovirus vector ChAdOx1, containing the full-length structural surface glycoprotein (spikeprotein) of SARS-CoV-2, with a tissue plasminogen activator leader sequence. ChAdOx1 nCoV-19 expresses a codon-optimisedcoding sequence for the spike protein(GenBank accession number MN908947). We did a phase 1/2 single-blind, randomised controlled trial of ChAdOx1 nCoV-19 compared with a licensedmeningococcal group A, C, W-135, and Y conjugate vaccine(MenACWY; Menevo, Nimenrix, Pfizer, UK), as control vaccine, in healthy adults in the UK.(See next study)
Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: a preliminary report of a phase 1/2, single-blind, randomised controlled trial Figure 1: Solicited local (A) and systemic (B) adverse reactions in first7 days after vaccinationas recorded in participant symptom electronic diaries. Fatigue and headachewere the most commonly reported systemic reactions. Fatiguewas reported in the ChAdOx1 nCoV-19 group by 340 (70%) participants without paracetamol
In the ChAdOx1 nCoV-19 group, antibodies against SARS-CoV-2 spike protein peaked by day 28 and remained elevated to day 56 Discussion Our preliminary findings show that the candidate ChAdOx1 nCoV-19 vaccine given as a single dose was safe and tolerated, despite a higher reactogenicity profilethan the control vaccine, MenACWY. Before vaccination, only one (1%) of 98 participants who were tested had high titre (>200) neutralising antibodies against ChAdOx1. Antibodies were detectable at a lower level in a further 18 (1%) participants, High levels of neutralising antibody at baseline seen in a small number of participants probably indicates prior asymptomatic infection, Importantly, there are accumulating data to suggest T-cell responses play an important role in COVID-19mitigation; individuals who were exposed but asymptomatic developed a robust memory T-cell response without symptomatic diseasein the absence of a measurable humoral response.[20–22] However, a boost in cellular responses was not observed following the second ChAdOx1 nCoV-19 dose. This is consistent with previous findingson viral vectored vaccines given as part of a homologous prime-boost regimen.[12] Additionally, the study findings are not easily generalisable, as this is a first-in-human study of fairly young and healthy volunteers, the majority of whom were white. Further studies are required to assess the vaccinein various population groups including older age groups, those with comorbidities, and in ethnically and geographically diverse populations. In conclusion, ChAdOx1 nCoV-19 was safe, tolerated, and immunogenic, while reactogenicity was reduced with paracetamol.
Declaration of interests SCG is co-founder and board member of Vaccitech(collaborators in the early development of this vaccine candidate) and named as an inventor on a patent covering use of ChAdOx1-vectored vaccines and a patent application covering this SARS-CoV-2 vaccine. TL is named as an inventor on a patent application covering this SARS-CoV-2 vaccine and consultant to Vaccitech. PMF is a consultanttoVaccitech. AJP is Chair of the UK Department of Health and Social Care’s Joint Committee on Vaccination & Immunisation (JCVI), but does not participate in policy advice on coronavirus vaccines, and is a member of the WHO Strategic Advisory Group of Experts (SAGE). SUMMATION/NOTES OF INTEREST Other vaccinestudies (now recruiting) involving ChAdOx1 85A Aerosol Versus Intramuscular Vaccinationin Healthy Adults (TB039) - Mycobacterium Tuberculosis, Protection Against Tuberculosis – Estimated completion: December 31, 2020 Personal comment: There is no mention of IL-2 and regulatory T-Cells promotion (T-regs) in this study, and humoral stimulation (adaptive) is not as important as innate cell-mediated immune responses. Just observing TH1 outcomes does not necessitate a positive stimulation without other compounds like IL-2 induced T-regs. More inflammatory TH2 responses would be expected