Download
1 / 104
1.04k likes | 1.25k Views
Head And Neck Cancer. Mostafa EL-Haddad Kasr El-Ainy Hospital Cairo University NEMROCK 2009. Category 1 Priority; Patients with the tumour types for which there is evidence that prolongation of treatment affects outcome, and who are being treated radically with curative intent.

E N D
Head And Neck Cancer Mostafa EL-HaddadKasr El-Ainy Hospital Cairo University NEMROCK2009
Category 1 Priority; Patients with the tumour types for which there is evidence that prolongation of treatment affects outcome, and who are being treated radically with curative intent. The data reviewed show very strong evidence that prolongation of overall treatment time affects treatment outcome or local tumour control (cure rates) in patients with the following tumours: • SCC of the head and neck region. • SCC cervix. • non-small cell carcinoma of lung (NSCLC). Guidelines for the Management of the Unscheduled Interruption or Prolongation of a Radical Course of Radiotherapy (2nd Edition. 2002).
MD Anderson series showed that completed combined treatment (Surgery+Radiotherapy) in 11 weeks is better than 11 to 13 weeks and more than 13 weeks is the worst.
Why Head And Neck Is Special • Very Complicated anatomy. • Many risk organ in a very narrow space. • Needs high precision. • Patients in very bad shape. • RCR report for priority.
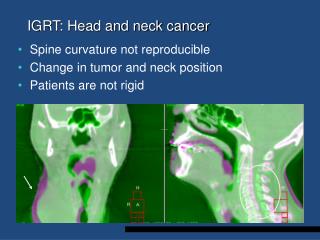
Imaging In Head and Neck Cancer • CT scan: Accurate information about pneumatization, integrity of bony structures. • MRI: soft tissue extension, Perineural, perivascular infiltration, intracranial extension. Base of skull CT? MRI?. Imaging before or after Biopsy? Larynx?
General Rules for Imaging • MR of choice in: Parotid, facial area, skull base (intracranial extension), Any tumor with potential perineural affection, oral cavity and oropharynx. • T2 WI excellent tumor to muscle enhancement. • T2 allows differentiation between secretions and mucosal thickening together with tumor which have low signal (Low water content). • In T1 look at the tumor invading Fat. (Fat shows high signal in T1).
CT is preferable if Swallowing may be a problem. (Ca Larynx). • DON’T FORGET NECK ULTRASOOUND. • PET and PET CT.
Thyroid. • Parotid. • Ear. • Eye and Orbit. • PNS. FORGET IT
Immobilization • Comfort and immobilization. • Unsightly setup marks. • Mask, Tape stretched, Beam directing shell. • Coughing, sneezing, respiration and swallowing. • Mark LNs. • Important land marks: (canthus, orbits, external auditory canal, oral commissures). • Before making the mask, use the fluoroscopy to align the patient and put him in the suitable position.
In Our Department • Put all head and neck patients on the C head rest. • PNS, Nasopharynx. (MAIN). • Ear, parotid: may be on patient side. • Pituitary in Flexion. • You can use hyperextension in any patient where you can protect the larynx .
Facial Mask system • Thermoplastic mask. • Beam directing shell. • Plastic material.
Radioopaque Markers And Stents • Wires to mark important structures or lymph nodes. • Stent to depress the tongue, protrude the lips.
Positioning • Mask on the Simulation, Why?
Positioning • Tilt your patient head ?? • Do you know what you did? You re tilting the gantry.
Positioning Bad alignment for your patient, Do you know what you are doing?? You are turning your couch
Head supports • Hyperextension can be achieved by elevating the chest without make a strain on the head.
A comfortable head support is one that tightly fits to the posterior surface of the head and neck and help the patient to maintain the position without straining. The neck is rested but not the head, this open room for a movement
Dental Impression • When you have to use tongue depressor?
Dental Impression • When the maxillary antrum is treated the Tongue and lower half of the mouth can be excluded. • Likewise, when a tumor of the tongue or the floor of the mouth are treated the upper part of the mouth can be excluded. • Used a dental impression material with a syringe inside for breathing.
Treatment Techniques Basic treatment technique: for the majority: • Two lateral and one lower anterior fields. • First including the spinal cord in phase I and then off cord for phase II.
Overlapping RegionProblem WHY IT’S A PROBLEM?
Ways To Solve this Overlap Method1: Midline spinal cord block in the anterior supraclavicular field. Against: Can not be done when anterior structures should be included in the field.
Ways To Solve this Overlap Method 2: Gap between two fields calculated by : ½ field1 length x depth/SSD + ½ field2 length x depth/SSD Against: High uncertainty.
Ways To Solve this Overlap Method 3: Put a block over the spinal cord at the posterior inferior angle of the lateral field. Against: Difficult set-up. Still there is lateral and anterior overlap
Still there is overlap in the lateral and anterior soft tissues? How can you solve it?
Ways To Solve this Overlap Method 4: Use Collimator and Couch angle. Against: Time consuming (table move only from inside the room). Errors in movement.
Anterior neck field Lateral head and neck field Overlap region