Download
1 / 21
220 likes | 371 Views
Primary and secondary prevention of osteoporotic fragility fractures in postmenopausal women. Implementing NICE guidance. 2008. NICE technology appraisal guidance 160 and 161. What this presentation covers. Definitions and scope Background Recommendations Costs and savings Discussion

E N D
Primary and secondary prevention of osteoporotic fragility fractures in postmenopausal women Implementing NICE guidance 2008 NICE technology appraisal guidance 160 and 161
What this presentation covers • Definitions and scope • Background • Recommendations • Costs and savings • Discussion • Find out more
Note: updated guidance • NICE reviews each piece of guidance it issues. • TA161 replaces NICE technology appraisal guidance 87 issued in January 2005. • The review and re-appraisal of alendronate, etidronate, risedronate, raloxifene and teriparatide for secondary prevention of osteoporotic fragility fractures has resulted in changes in the criteria for offering these drugs. • In addition, strontium ranelate has alsobeen appraised.
Definitions • BMD: bone mineral density • DXA: dual-energy X-ray absorptiometry • Fragility fracture: a low-trauma fracture • T-score: the number of standard deviations (SD) below the mean BMD of young adults at their peak bone mass • Osteoporosis: a T-score of −2.5 (SD) or below on DXA scanning
Scope • For the purposes of this guidance: • Primary prevention refers to opportunistic identification, during visits to a healthcare professional for any reason, of postmenopausal women who are at risk of osteoporotic fragility fractures and who could benefit from drug treatment. It does not imply a dedicated screening programme. • Secondary prevention relates only to treatments for the secondary prevention of fragility fractures in postmenopausal women who have osteoporosis and have sustained a clinically apparent osteoporotic fragility fracture.
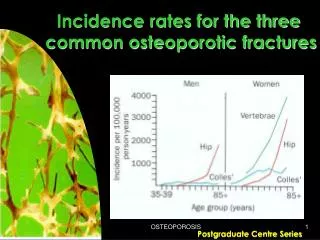
Background • In England and Wales, it is estimated that: • over 2 million women have osteoporosis • 180,000 osteoporosis-related fractures occur annually • 1 in 3 women over 50 years of age will sustain a vertebral fracture • 2 million bed days annually are a result of fractures • annual social and hospital care costs £1.8 billion
Clinical need • Fragility fractures are the clinically apparent outcome of osteoporosis. • In the absence of fracture, osteoporosis is asymptomatic. • Hip fractures are associated with increased mortality. • 50–70% of vertebral fractures do not come to clinical attention.
Risk factors and risk assessment Independent clinical risk factors for fracture: • parental history of hip fracture • alcohol intake of 4 or more units per day • rheumatoid arthritis. Indicators of low bone mineral density: • low body mass index below 22 kg/m2 • ankylosing spondylitis • Crohn’s disease • conditions resulting in prolonged immobility • untreated premature menopause.
Technologies • Alendronate, etidronate, risedronate (bisphosphonates)inhibitors of bone resporption and increase BMD by alteringosteoclast activation and function. • Raloxifene (selective oestrogen receptor modulator)SERMs have selective activity in various organ systems, acting aseither a weak oestrogen-receptor agonist or antagonist. Strontium ranelatean element with properties similar to calcium with a dual effecton bone metabolism, increasing formation and decreasing resorption. • Teriparatide (parathyroid hormone)a recombinant fragment of human parathyroid hormonewhich stimulates new formation of bone and increasesresistance to fracture.
Adherence to treatment • Contraindications • Compliance with special instructions for administration • Intolerance • Bisphosphonates (alendronate, etidronate, risedronate) – persistent upper gastrointestinal disturbance that is sufficiently severe to warrant discontinuation of treatment, where instructions for administration have been followed correctly • Strontium ranelate – persistent nausea or diarrhoea, which warrants discontinuation of treatment
Primary prevention: first treatment option • Initial treatment offered: alendronate
Primary prevention: alternative treatment option (1) • Alternative treatment – risedronate or etidronate when women: • are unable to comply with administration of, or have a contraindication to or are intolerant of alendronate and • have a combination of T-score, age and number of clinical risk factors as outlined in the table.
Primary prevention: alternative treatment option (2) • Alternative treatment – strontium ranelate when women: • are unable to comply with administration of, or have a contraindication to or are intolerant of alendronate and either risedronate or etidronate and • have a combination of T-score, age and number of clinical risk factors as outlined in the table.
Secondary prevention: first treatment option • Initial treatment offered: alendronate • Postmenopausal women with confirmed osteoporosis • A DXA scan may not be required in women aged 75 or over
Secondary prevention: alternative treatment option (1) • Alternative treatment – risedronate or etidronate when women: • are unable to comply with administration of, or havea contraindication to or are intolerant of alendronate and • have a combination of T-score, age and number of clinical risk factors as outlined in the table.
Secondary prevention: alternative treatment option (2) • Alternative treatment – strontium ranelate or raloxifene when women: • are unable to comply with administration of, or havea contraindication to or are intolerant of alendronate and either risedronate or etidronate and • have a combination of T-score, age and number of clinical risk factors as outlined in the table.
Secondary prevention: alternative treatment option (3) • Alternative treatment – teriparatide when women: • are unable to take, have a contraindication to or are intolerant of alendronate and either risedronate or etidronate, or • have a contraindication to, or are intolerant of strontium ranelate or • have had an unsatisfactory response to treatment with alendronate, risedronate or etidronate and • have a combination of T-score, age and number of fractures as outlined in the table.
Clinical management • Women currently receiving treatment that is not recommended in this guidance should have the option to continue treatment. • It is assumed women who receive treatment have an adequate calcium intake and are vitamin D replete– consider supplements if needed.
Costs and savingsPrimary and secondary preventionper 100,000 population
For discussion • How/or will current local prescribing arrangements need to change as a result of this guidance? • How can we increase adherence to therapy? • What arrangements currently exist regarding access to DXA scanning for this patient group? • How can we improve links between primary and secondary care to improve the care of women with osteoporosis?
Find out more • Visit www.nice.org.uk/TA160and www.nice.org.uk/TA161 for: • Other guidance formats • Costing report and template • Audit support