Download
1 / 31
470 likes | 3.39k Views
Cytomegalovirus infection. Presented by: Dr.D. Al-Masri. Moderated by:Dr.Y.Abu-Osbaa’. Introduction. It is the most common congenital infection in USA. It is a leading cause of hearing loss,mental retardation, and cerebral palsy. It is an opportunistic pathogen in Immunocompromised.

E N D
Cytomegalovirus infection Presented by: Dr.D. Al-Masri. Moderated by:Dr.Y.Abu-Osbaa’.
Introduction • It is the most common congenital infection in USA. • It is a leading cause of hearing loss,mental retardation, and cerebral palsy. • It is an opportunistic pathogen in Immunocompromised.
Introduction • It is a double stranded DNA virus. • It is the largest member of herpesviridae family.. • Exit the cells by pinocytosis. • Restriction endonuclease.
Epidemiology • The prevalence of CMV infection and the age at first infection vary according to living conditions,child rearing practices, and sexual behavior. • Virus is present in saliva,tears,semen,urine,cervical secretions, and blood for months to years after initial infection as well as the milk of seropositive mothers.
Epidemiology • It has a worldwide distribution. • Prevalence: • Health care providers are not at increased risk of infection from patients.
Epidemiology • It is transmitted via direct contact with body fluids, intimate contact, care of young children, blood transfusion, and organ transplant. • Congenital CMV infection occurs in approximately 0.5% to 1.5% of births. It is well known that CMV can be transmitted to the fetus even when maternal infection occurred long before conception.
Epidemiology • It occurs in immune mothers due to reactivation of latent virus during pregnancy ,chronic infection, or reinfection with a new strain. • When primary infection occurs during pregnancy the risk of transmission to the fetus is 35%. It occurs either by sexual contacts or contact with young children regardless of the gestational age. • Intrapartum transmission or transmission by human milk occur more commonly than congenital infection. • Infants who acquire the virus shed it in saliva and urine for years.
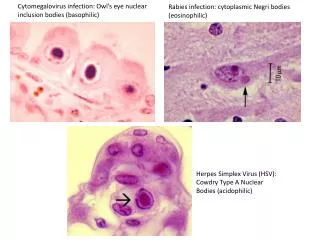
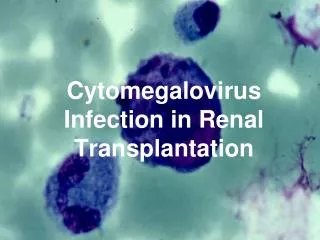
Pathogenesis • CMV is large complex virus that has 20 times the genetic material of HIV with DNA sequences encoding more than 100 proteins. • The infection occurs due to impairment of T-cell immunity. • Cytomegalic cells: pathognomonic.
Pathogenesis • Important features in pathogenesis: • Ability of the virus to destroy host cells. • Ability to infect wide range of cells and tissues . • Ability to to evade and interfere with host defense mechanisms. • Ability to persist indefinitely in the host.
Pathogenesis • Impaired organ function results from combination of lytic infection of cells and vascular compromise . • Dissemination is due to infection of WBC and vascular endothelial cells. • A small proportion of circulating monocytes in seropositive persons harbor latent CMV.
Pathogenesis • The ability of the virus to maintain active infection is due to: • Inhibition of host cytotoxic T-lymphocyte responses by interference with processing and presentation of viral antigens by MHC class I molecules. • Interference with helper T-cell responses by degradation of MHC class II molecules. • Inhibition of killing by natural killer cell. • Interference with apoptosis and complement-mediated lysis or sequestration of chemokines.
Clinical manifestations • Mostly asymptomatic. • CMV accounts for 50% of cases of heterophile-negative mononucleosis. • Differ from EBV? • Fever and malaise often persist for more than 2 weeks. • The expected outcome is complete recovery. • Rare complications: peripheral neuropathy, hemolytic anemia, thrombocytopenia, pneumonia, retinitis, gastrointestinal ulceration and encephalitis.
Congenital CMV infection • More than 90% of children have no clinical evidence of disease as newborns. • Lab abnormalities reflect involvement of hepatobiliary , hematopoeitic and CNS. • Newborns with symptomatic infection have wide range of severity. • Mortality is 10-15% • Among symptomatic survivors, neonatal clinical abnormalities can be expected to resolve within weeks except for those involving CNS and hearing.
Outcome • Mental retardation. • Hearing loss 7-15% in initially asymptomatic newborn • Cerebral palsy. • Retinal damage.
Congenital CMV infection • Factors associated with increased risk of CNS sequel: • Primary maternal infection during pregnancy. • Abnormal neurologic examination findings. • Microcephaly. • Brain C.T.scan abnormalities. • Increased CSF protein. • Chorioretinitis.
Perinatal/Neonatal CMV infection • It is not associated with newborn illness or CNS sequel, except perhaps in very preterm newborns who have very low levels of passively acquired antibody at the time of infection and they may be left with residual neurologic sequelae & psychomotor retardation. • It is not associated with increase hearing loss, chorioretinitis or microcephaly. • Transfusion acquired CMV to newborns whose mothers are seronegative can cause a picture similar to congenital infection and presents with jaundice, hepatosplenomegaly, abnormal liver function, thrombocytopenia, hearing loss and pulmonary problems.
Differential diagnosis in the newborn • TORCHS. • Acute viral ,bacterial or systemic fungal infections. • In born errors of metabolism can cause neonatal hepatitis,thrombocytopenia , hepatosplenomegaly , encephalopathy and anemia.
CMV in Immunocompromised children • The majority are due to reactivation of the host CMV and these often are clinically silent. • When primary infection occurs by blood products and transplanted organ, it is usually associated with disease. • The clinical manifestation correlates with the degree of immunologic impairment. • Primary CMV infection in transplant patients frequently is heralded by fever and leucopoenia, rash, arthralgia and elevated serum alanine aminotransferase levels.
CMV in Immunocompromised children • Complications in transplant patients: • Impaired function of the transplanted organ. • Pneumonitis, G.I. Ulceration, hepatitis. • Opportunistic fungal infection.
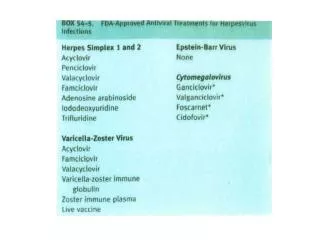
CMV in Immunocompromised children • Complications in AIDS patients: • Retinitis. • Esophagitis , Colitis , Hepatitis. • Encephalitis,peripheral neuropathy. • Pneumonitis. • Treatment is palliative requiring therapy with Ganciclovir, Foscarnet or Cidofovir followed by maintenance therapy with one of these drugs which is continued indefinitely or until the patient immune function improves and stabilizes.
Laboratory diagnosis • Congenital CMV infection is diagnosed by : • Detection of virus in the urine or saliva of a newborn • PCR. • CMV IgM: transient. • Detection of CMV within the first 3 weeks of life is considered proof of congenital CMV but after this period it is not certain if it is due to prenatal or perinatal infection. • Viremia demonstrated by buffy coat or DNA indicates active infection.
Laboratory diagnosis • Diagnosis of CMV infections in immunocompromised patients is much more difficult. • Serology is of limited value. • CMV IgG is a good marker for past infection and identifies the problematic positive donor/negative recipient situation that carries a high risk for primary infection and CMV disease in the immediate post transplant period.
Laboratory diagnosis • Detection of CMV in blood is a much better predictor of disease among immunocompromised patients than is shedding of virus. • Quantitative tests has good correlation with the clinical picture either by detection of WBC positive for CMV antigens by immunofluorescence or quantitative PCR.
Laboratory diagnosis • Congenital infection: • Virus isolation. • IgG • IgM
Management • Antiviral treatment: has reduced the burden of CMV disease substantially in immunocompromised patients. • Ganciclovir, Foscarnet, and Cidofovir. • No antiviral agent is approved for treatment of congenital CMV infection but………. • Side effects include neutropenia , thrombocytopenia , liver dysfunction ,reproductive toxicity and carcinogenicity.
Management • The approach to antiviral treatment in immunocompromised patients can vary with • The clinical settings. • The type of CMV infection. • Clinical manifestations of CMV disease. • Laboratory evidence of CMV infection. • Degree of immunosuppression.
Prevention • All preschool-age children should be considered potential sources of infection. • Avoid contact with body fluids from young children and careful hand washing • Educating women before getting pregnant. • Vaccination. • Limit transfusion-acquired CMV infection. • Prophylactic antiviral treatment and passive immunization to prevent CMV disease after transplantation.