Download
1 / 51
580 likes | 1.44k Views
Oral Mucosa. Dr. Ali Tahir. Mucous membrane. Moist lining of GIT, Nasal passages & body cavities that communicate with the exterior The mucous membrane of oral cavity is called “Oral Mucosa” Located anatomically between skin & GIT mucosa & shows some properties of both

E N D
Oral Mucosa Dr. Ali Tahir
Mucous membrane Moist lining of GIT, Nasal passages & body cavities that communicate with the exterior The mucous membrane of oral cavity is called “Oral Mucosa” Located anatomically between skin & GIT mucosa & shows some properties of both Because of its various functions, it is considered an organ Dr. Ali Tahir, M.Phil (Part I)
Functions of Oral Mucosa • Protection • From mechanical forces & abrasion while chewing food & from micro-organisms resident in the oral cavity • Sensation • Temperature, Touch, Pain, Taste • Receptors for Satisfaction of thirst, Swallowing, gagging, salivation • Secretion • Major secretion is saliva • Major & minor salivary glands • Sebaceous glands are frequently present (upper lip & buccal mucosa) sometimes called Fordyce’s spots but their secretions are insignificant • May be an accident of embryologic development Dr. Ali Tahir, M.Phil (Part I)
Anatomy Two parts • Outer vestibule (bounded by lips & cheeks) • Oral cavity proper (separated from vestibule by teeth & gingiva) • Superiorly bound by hard & soft palate • Inferiorly by floor of mouth & tongue • Posteriorly by pillars of fauces Dr. Ali Tahir, M.Phil (Part I)
Types • Lining Mucosa • Constitutes the large part (60%) • Soft, pliable • Masticatory mucosa • 25% • Firm, immobile • Gingiva & hard palate • Specialized mucosa • Dorsum of tongue, in the form of papillae • Unique to oral cavity • 15% Dr. Ali Tahir, M.Phil (Part I)
Clinical features • Oral mucosa is more deeply coloured compared to skin • B/c of • Concentrated & dilated blood vessels • Thickness of epithelium • Degree of keratinization • Amount of melanin • Inflamed mucosa is more red b/c of dilation of blood vessels Dr. Ali Tahir, M.Phil (Part I)
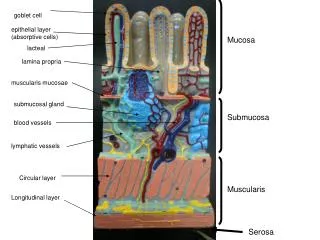
Components • Two main components • Stratified Squamous Epithelium (oral Epithelium) • Lamina Propria • Interface b/w these two is irregular consisting of C.T papillae & rete ridges/pegs • Basal lamina separates the two Dr. Ali Tahir, M.Phil (Part I)
Types & Layers of Epithelium Keratinized Epithelium Hard palate gingiva & tongue • Basal cell layer • Prickle cell layer • Granular cell layer • Keratinized layer Non-keratinized Epithelium Buccal mucosa, floor of mouth, ventral surface of tongue • Basal cell layer • Prickle cell layer • Intermediate cell layer • Superficial cell layer Dr. Ali Tahir, M.Phil (Part I)
Submucosa A layer of loose fatty or glandular connective tissue may be present between the oral mucosa & underlying bone/muscle This layer contains blood vessels, nerves & minor salivary glands Composition of submucosa determines the flexibility of the attachment of oral mucosa to underlying stuructures Eg, in gingiva & hard palate, oral mucosa is directly attached to periosteum & no submucosa is present. This is called mucoperiostium & is firm and inelastic Dr. Ali Tahir, M.Phil (Part I)
Lymphoid tissue • In several regions, nodules of lymphoid tissue consisting of crypts formed by invaginations of the epithelium into the lamina propria are present • Mostly present in posterior parts of oral cavity • Lingual tonsils • Palatine tonsils • Pharyngeal tonsils • Together form Waldeyer’s ring • Small nodules may also be present in soft palate, ventral surface of tongue & floor of mouth Dr. Ali Tahir, M.Phil (Part I)
Oral epithelium • Consist of tightly packed cells called keratinocytes • Maintains its structural integrity by a continuous process of cell renewal • Two types of cell population • Progenitor cells • Maturing cells • Cells produced by mitosis in the deeper layers (basal & parabasal layers) migrate to the surface layers Dr. Ali Tahir, M.Phil (Part I)
Epithelial proliferation • Dividing cells are present in clusters at the bottom of epithelial ridges • Progenitor population consists of two groups • Stem cells (slow cell cycle) • Produce basal cells & retain proliferative potential of tissue • Amplifying cells • Increase the no. of cells available for maturation • After division, each daughter cell recycles in the progenitor population or enters the maturing population • Time required to replace all the cells in the epithelium is called Turnover time Dr. Ali Tahir, M.Phil (Part I)
Turn over time Wide range of estimates have been made 52-75 days for skin 4-14 days for gut 41-57 days for gingiva 25 days for cheek Non-keratinized epithelium turns over faster than the keratinized Dr. Ali Tahir, M.Phil (Part I)
Significance • Cancer chemotherapy drugs block the life cycle of cancer cells as well as normal host cells • Cells with short turnover time are most affected. These include • Blood cells precursors in bone marrow • Intestinal epithelium • Oral epithelium • Leads to formation of oral ulcers • In addition, inflammation also affects rate of mitosis Dr. Ali Tahir, M.Phil (Part I)
Factors influencing the epithelial proliferation Epidermal growth factor Keratinocyte growth factor Interleukin-1 Transforming growth factor α and ß Dr. Ali Tahir, M.Phil (Part I)
Keratinization Present on masticatory mucosa (hard palate, gingiva, parts of dorsal surface of tongue) Inflexible, tough, abrasion resistant, tightly bound to lamina propria Process of maturation is called keratinization or cornification Dr. Ali Tahir, M.Phil (Part I)
Keratinization Basal cell layer (stratum basale) Cuboidal or columnar cells containing bundles of tonofibrils. Site of most cell divisions Prickle cell layer (stratum spinosum) Larger, ovoid cells with conspicoustonofibril bundles, upper part of layer contains membrane-coating granules Granular cell layer (Stratum granulosum) Flattened cells, keratohyaline granules associated with tonofibrils Keratinized (stratum corneum) Extremely flattened & dehydrated cells with loss of all organells, cells filled with fibrillar material. If pyknoticnuclie retained, called para-keratinized Dr. Ali Tahir, M.Phil (Part I)
Non-keratinized Basal cell layer (stratum basale) Cuboidal/columnar cells containing separate tonofilaments Prickle cell layer (stratum spinosum) Larger ovoid cells containing dispersed tonofilaments, membrane coated granules in upper part of layer Intermediate layer (stratum intermedium) Slightly flattened cells containing dispersed tonofilaments & glycogen Superficial layer (stratum superficiale) Slightly flattened cells, dispersed tonofilaments, glycogen, fewer organelle, nuclie Dr. Ali Tahir, M.Phil (Part I)
Ultra structure of epithelial cells Cells of basal layer are least differentiated cells Contain organelles & certain structures such as tonofilaments & desmosomes Tonofilaments are fibrous proteins & belong to the class of intermediate filaments Aggregate to form bundles called tonofibrils Chemically represent cytokeratins which are chracteristic constituents of epithelial cells Dr. Ali Tahir, M.Phil (Part I)
Keratins • Represent a large family of proteins • Classified according to the molecular weight & charge. E.g.. • Low molecular weight (40kDa) found in glandular & simple epithelia • Intermediate molecular weight found in stratified epithelia • High molecular weight (67kDa) in keratinized stratified epithelia • Keratinzed epithelium has • Type1, 5, 6, 10, 14, 16 • Non-keratinized epithelium has • Type 4, 5, 13, 14, 19 Dr. Ali Tahir, M.Phil (Part I)
Adhesions & Attachments Cohesion b/w cells is provided by protein-carbohydrate complexes produced by epithelial cells themselves In addition, modifications of adjacent cell membranes of cells called desmosomes provide attachment into which tonofilaments insert Adherence b/w epith & C.T is provided by hemidesmosomes which attach the cells to basal lamina Dr. Ali Tahir, M.Phil (Part I)
Adhesions & Attachments • Two other types of connections are • Gap junctions • Tight junctions • Gap junction: • Membranes of adjacent cells run closely together separated by a small gap • Small interconnections are present • Gap junctions allow electric/chemical communication • Tight junction • Adjacent cell membranes are tightly apposed Dr. Ali Tahir, M.Phil (Part I)
Membrane-coated granules Also called lamellate granules Are small memrane bound structures about 250nm in size containing glycolipid, originate from golgi complex Appear in the upper part of prickle layer They are elongated in keratinized & circular in non-keratinized epithelium In the upper part of stratum granulosum/intermedium, these granules appear to fuse with superficial cell membrane to discharge their contents into intercellular space Dr. Ali Tahir, M.Phil (Part I)
Cell Maturation in Keratinized epith Cells in the superficial part of granular layer develop a thickening on the intra-cullular aspect of their membrane It contributes in resistance of keratinized layer to chemical solvents One of the major constituent of this thickening is a protein called involucrin Dr. Ali Tahir, M.Phil (Part I)
Granular layer Found in keratinized epithelium Contains keratohyalin granules, which are basophilic granules under light microscope These are irregular in shape 0.5-1nm in size Synthesized by ribosomes Intimately associated with tonofibrils Facilitate aggregation & formation of cross-links b/w cytokeratin filaments Proteins making bulk of these granules are called Loricrin Dr. Ali Tahir, M.Phil (Part I)
Squames As the cells of granular layer reach the junction with the keratinized layer, a sudden change occurs All organelles are lost, including nuclie & keratohyalin granules Cells dehydrate & assume the shape of hexagonal disks These are called squames Squames are lost within days, a process called desquamation & replaced by cells from underlying layers Limit the colonization of pathogenic micro-organisms Keratin layer in oral cavity may be upto 20 layers of squames Dr. Ali Tahir, M.Phil (Part I)
Cell maturation in non-keratinized epithelium A slight increase in size occurs in intermediate cell layer Accumulation of glycogen in cells of surface layer Occasionally keratohyalin granules are seen but these aren’t associated with tonofilaments These granules may remain upto the surface layer Dr. Ali Tahir, M.Phil (Part I)
Non-keratinized epithelium Cells in the superficial layer are slightly more flattened Contain dispersed tonofilaments, retain nuclie & do not dehydrate Thus are tolerant to compression & distension Dr. Ali Tahir, M.Phil (Part I)
Anatomical variations Some variation of anatomical locations of keratinized & non-keratinized epithelium may occur Hyperkeratosis of keratinized oral epithelium is physiological to chronic irritation Hyperkeratosis of non-keratinized epithelium can be associated with abnormal cellular changes that can lead to cancer Inflammation of gingiva can lead to loss of keratinization or parakeratinization These changes are usually reversible when irritant is removed Dr. Ali Tahir, M.Phil (Part I)
Permeability & absorption of oral epithelium Oral epithelium is largely impermeable & lacks absorptive capacity Epithelium at the floor of the mouth, however, is thin & more permeable comparatively (Nitroglycerin to relieve angina pain) Oral epithelium thus limits the absorption of toxins from micro-organisms except in dentogingival junction Dr. Ali Tahir, M.Phil (Part I)
Other cells in oral epithelium • Melanocytes • Present in basal layer • Lack desmosomes & tonofilaments • Dendritic, synthesis of melanin pigment granules (melanosomes) • Merkel Cells • Present in basal layer • Non-dendritic, tactile sensation • Langerhans cells • Dendritic • Present in parabasal layer • Antigen trapping & processing • Lymphocytes • Variable location • Inflammatory response • B or T cells Dr. Ali Tahir, M.Phil (Part I)
Pigmentation • Two types of pigmentation is seen in oral mucosa • Endogenous • Exogenous • Endogenous pigments in oral mucosa are melanin & hemoglobin • Melanocytes are derived from neural crest ectoderm • Enter the epithelium at 11th week of gestation • Melanosomes are injected into adjacent keratinocytes by long dendritic processes that often pass through several layers of epithelium • Groups of melanosomes can be seen under light microscope, called melanin granules Dr. Ali Tahir, M.Phil (Part I)
Pigmentation Light & dark individuals have the same number of melanocytes, the difference results from the activity of melanocytes In persons with heavy melanin pigmentaion, melanophages are seen in the connective tissue In oral mucosa, melanin pigmentation is most commonly seen in gingiva, buccal mucosa, hard palate & tongue & is more in dark skinned individuals Dr. Ali Tahir, M.Phil (Part I)
Pigmented pathologies • Oral melanoticmacule • Increased production of melanin pigment without proliferation of melanocytes • Nevus (Mole) • Benign proliferation of melanocytes • Melanoma • Malignant tumour of melanocytes • Melanoma of oral cavity is aggressive Dr. Ali Tahir, M.Phil (Part I)
Pigmentation • Exogenous • Caused by foreign material introduced locally or systemically • One of the most common oral exogenous pigment is amalgum • Gives rise to bluish-gray patch called amalgum tattoo • Systemic administration of metals such as lead & bismuth can cause gingival margin pigmentation (called Burton’s line) Dr. Ali Tahir, M.Phil (Part I)
MCQs Stratum distendumis another name for Submucosa of lining oral epithelium Prickle layer of non-keratinized epithelium Superficial layer of Non-keratinized epithelium Granular layer of keratinized epithelium Dr. Ali Tahir, M.Phil (Part I)
MCQs The superficial cells of granular layer of keratinized oral epithelium have intra-cellular thickenings to resist chemical solvents containing which proteins? Cytokeratins Glycoproteins Involucrin Filaggrin Dr. Ali Tahir, M.Phil (Part I)
MCQs Blood flow in oral mucosa is the greatest in which region Soft palate Floor of mouth Gingiva tongue Dr. Ali Tahir, M.Phil (Part I)
MCQs In infants, Suckling Pad refers to A thickened vermillion zone A thickened intermediate zone A thickened labial mucosa A thickened muco-cutaneous junction Dr. Ali Tahir, M.Phil (Part I)
MCQs Dr. Ali Tahir, M.Phil (Part I)