Download

1 / 40
400 likes | 569 Views
Mycobacterium kansasii , species or complex? Genetic and epidemiological insights. Enrico Tortoli Regional Reference Center for Mycobacteria Florence - Italy. Congress of Japanese Society of Tuberculosis – Kurashiki, April 25, 2003. Brief history of M. kansasii.

E N D
Mycobacterium kansasii,species or complex?Genetic and epidemiological insights Enrico Tortoli Regional Reference Center for Mycobacteria Florence - Italy Congress of Japanese Society of Tuberculosis – Kurashiki, April 25, 2003
Brief history of M. kansasii • 1953: description by Buhler & Pollak • 1960-70: most common NTM causing infections in USA and UK • 1980s: surpassed by M. avium as cause of pulmonary disease; isolations on the rise in Japan • early 1990s (pre-HAART era): not rare, although far less common than M. avium as cause of pulmonary or disseminated disease in AIDS • late 1990s (HAART era): very rare in AIDS, more frequent in immuno-competent patients
Phenotypic characteristics of M. kansasii • Large cross-barred bacilli • Prevalently rough colonies • Photochromogenic • Slow growth at 30-40°C • Nitrate, Tween 80 hydrolysis, catalase and urease are positive • Arylsulfatase and tellurite are negative
Mycobacterium kansasii, a significant pathogen • Annual rate of infection in general population ranges from 0.5 to 1 per 100,000 • Significant geographical variability is observed • rare in Australia and Japan • very frequent in Louisiana (USA) and Czech Republic • Culturing of M. kansasiifrom human sources is not proof of disease; 1/3 of respiratory isolates represent colonization rather than infection
Diseases inimmunocompetent patients • Pulmonary disease • preexisting lung disease • pneumoconiosis • chronic obstructive pulmonary disease • impaired ventilation function • Lymphadenitis (childhood) • Soft tissues infection • Cutaneous lesions • Bone and joint disease • Genitourinary disease • Disseminated disease
Other risk factors • Exposure to dust • Cancer • Alcoholism • Smoke • Systemic illness • Exposure to M. kansasii -contaminated water • Hyperendemic geographic areas
Disease inimmunodeficient patients • Disseminated disease • low CD4 level • Pulmonary disease
Therapeutic hints • The key antimicrobial, rifampin, is mostly used in association with ethambutol and with a 3rd drug (streptomycin, isoniazid or amikacin) • ATS recommends 18 month therapy
M. kansasii in the environment • Frequently isolated from both drinking and natural water • Rarely isolated from soil
First reported variants of M. kansasii • Clinically significant strains • semiquantitative catalase > 30 mm • high virulence in guinea pig • Strains with doubtful significance • semiquantitative catalase < 30 mm • low virulence in guinea pig (Wayne, 1962)
Genetic targets of M. kansasii • 16S rRNA gene • 16S-23S internal transcribed spacer • 65kD heat shock protein gene • Repetitive DNA sequences • girA intein-coding sequence
DNA probe developed for M. kansasii • Research tools • pMK1-9 • undetermined DNA region • p6123 • undetermined DNA region • Commercial tools • AccuProbe (2 formulations) • 16S rRNA • INNO LiPA MYCOBACTERIA • ITS
pMK1-9 DNA probe • Hybridization with all M. kansasiitested (Huang et al., 1991) • Hybridization failed by 20 out of 105 M. kansasiiisolates (Ross et al., 1992)
p6123 DNA probe • Hybridization with all M. kansasiitested (Yang et al., 1993)
AccuProbeM. kansasii • AccuProbe (1st formulation) hybridizes with all pMK1-9-positiveM. kansasiibut with only a part of pMK1-9-negative ones (Ross et al., 1992) • Only 50, out of 69 M. kansasiiisolates, hybridize with the 1st AccuProbe (Tortoli et al., 1994) • The reformulated AccuProbe hybridizes also with the strains negative with the previous version (Tortoli et al., 1996)
INNO LiPA MYCOBACTERIA • 3 line-probes are addressed to the identification of differentM. kansasiistrains • all the strains positive with the 1st AccuProbe hybridize with line MKA-1 • all the strains negative with the 1st and positive with the 2nd AccuProbe hybridize with line MKA-2 • the strains negative with both AccuProbe hybridize with line MKA-3 (Tortoli et al., 2001)
Genetic sequencing • The strains pMK1-9-negative differ 5 nucleotides in the 16S rDNA from the pMK1-9-positive ones (Ross et al., 1992) • 1 to 6 nucleotide diversity differentiates, in the first 500 bp of 16S rDNA, 5 sequevars of M. kansasii(RIDOM) • Extensive diversities (12 to 49 nucleotides) characterize, in ITS, 5 sequevars of M. kansasii(RIDOM)
Repeated DNA sequences • GC-rich repetitive sequence • IS1652 • Major Polymorphic Tandem Repeat
Fingerprinting techniques • Restriction Fragment Length Polymorphism • the total bacterial DNA is digested with restriction enzymes • the fragments are separated by electrophoresis • Amplified Fragment Length Polymorphism • the total bacterial DNA is digested with restriction enzymes • oligonucleotide adapters are added by ligase • adapter-containing fragments are selectively amplified • amplification products are separated electrophoretically • Pulsed Field Gel Electrophoresis • large restriction fragments are obtained from total bacterial DNA • the fragments are separated by pulsed field electrophoresis • PCR Restriction Analysis • a PCR-amplified DNA sequance is digested with restriction enzymes • the fragments are separated by electrophoresis
GC-rich repetitive sequence • A repetitive sequence, with high guanosine and cytosine content, is present, in at least 30 copies, in M. kansasii, M. tuberculosis and M. szulgai and is responsible of polymorphism(Ross et al., 1992)
IS1652 • IS1652 is present in pMK1-9-negative M. kansasii only (Yang et al., 1993) • In such strains the number of copies, which ranges from 1 to 11, is responsible for significant polymorphism
Major Polymorphic Tandem Repeat • The MPTR consists of short tandemly repeated sequences of 10 bp separated by 5-bp spacers GCCGGTGTTG • About 80 different MPTR-containing regions are present in the mycobacterial genome • MPTR is present in M. tuberculosis complex, M. gordonae, M. gastri, M. kansasii, M. szulgai • A wide polymorphism characterizes the MPTR‑containing restriction fragments of M. kansasii(Hermans et al., 1992)
MPTR-based RFLP • pMK1-9-positive M. kansasiishare most bands in common; pMK1-9-negative strains are more heterogeneous (Ross et al., 1992) • AccuProbe-1-positive M. kansasiiexhibit a 3kb fragment; AccuProbe-1-negative strains present fragments of variable length (Yang et al., 1993)
Intein-coding sequences • Inteins are protein sequences that are excised from the precursor protein during maturation • Intein-coding sequences may be present in gyrA, the gene encoding for the A subunit of mycobacterial DNA gyrase • Several mycobacterial species present in gyrA an intein-coding sequence, others species do not • M. kansasii, M. flavescens and M. gordonae are the only species in which strains with and without gyrA intein are present (Sander et al., 1998)
Minor genetic heterogeneity • The gene encoding for the MPB70 protein-analogue of M. kansasiipresents sequence variations suggesting the heterogeneity of the species (Wooldford et al., 1997) • The amplification of ITS from different M. kansasiistrains reveals three different product profiles, in other mycobacterial species the profile is reproducible (Abed et al., 1995)
Tortoli et al., 1994 • AccuProbe-1-positive strains, differently from -negative ones, rapidly hydrolyze Tween 80 and possess alpha‑fucosidase activity • AccuProbe-positive and -negative strains cannot be distinguished by means of HPLC analysis • The isolation of AccuProbe-1-negative M. kansasiiis significantly more frequent (P=0.00007) from HIV‑positive than from HIV‑negative patients
Picardeau et al., 1997 (1/2) • RFLP, using MPTR as a probe, reveals 5 clusters • AFLP reveals multiple patterns clustering in 5 minor groups according to the ones of MPTR • RFLP reveals IS1652 in 2 of the above clusters, with a single copy and with 4-6 copies respectively; IS1652 is on the contrary missing in the others • PFGE reveals a number of patterns clustering in 5 major groups • PRA of hsp65 gene reveals 5 clusters
Picardeau et al., 1997 (2/2) • Cluster I includes typical M. kansasiiand is AccuProbe-1-positive • Clusters II to IV are AccuProbe-1-negative • Clusters V is AccuProbe-1-positive • Clusters II and III are closely related
Alcaide et al., 1997 (1/2) • PRA of hsp65 generate 5 different patterns • type I is AccuProbe-1-positive • types II and IV are AccuProbe-1-negative • types III and V are weakly AccuProbe-1-positive • gyrA intein is present in types I, IV and V while it lacks in II and III • Partial 16S rDNA sequence reveals 2 sequevars presented by types I, IV and V and by types II and III respectively • ITS sequence reveals 5 sequevars correlating with the hsp65 PRA types • PFGE of the digested chromosomal DNA generates 10 to 15 large fragments • moderate polymorphism in type I (clonal structure) • significant polymorphism in type II
Alcaide et al., 1997 (2/2) • Types I and II constitute frequent clinical isolates • Type I, differently from II, is almost absent in the environment • Types III, IV and V are rare in humans and frequent in the water
The five “types” of M. kansasii a S, single pattern; M, multiple patterns b 4 subgroups c 5 subgroups d 3 subgroups
The five “types” of M. kansasii a S, single pattern; M, multiple patterns b 4 subgroups c 5 subgroups d 3 subgroups
The five “types” of M. kansasii a S, single pattern; M, multiple patterns b 4 subgroups c 5 subgroups d 3 subgroups
The five “types” of M. kansasii a S, single pattern; M, multiple patterns b 4 subgroups c 5 subgroups d 3 subgroups
The five “types” of M. kansasii a S, single pattern; M, multiple patterns b 4 subgroups c 5 subgroups d 3 subgroups
The five “types” of M. kansasii a S, single pattern; M, multiple patterns b 4 subgroups c 5 subgroups d 3 subgroups
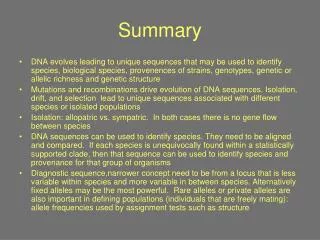
Taxonomic speculations • M. kansasii is • a single systematic entity? • a single species split in several subspecies? • complex including multiple species? • Evidence exists that, as a consequence of the high degree of divergence, several M. kansasiitypes are more closely related to other species than to each other
M. gordonae M. tuberculosis M. marinum M. ulcerans M. gastri } M. kansasii ii M. szulgai ITS-based phylogenetic tree M. kansasii iii M. kansasii v M. kansasii iv M. kansasii i
Epidemiological insights • Types I and II include all the significantly pathogen isolates • Type I presents a clonal structure • adaptation to human host? • divergence restricted by virulence properties? • it includes practically al M. kansasii pathogens for immunocompetent people (the high catalase producers of Wayne, and almost all the AccuProbe-1-positive strains) • Type II is rare in immunocompetent patients and frequent in HIV-infected ones • lower ability to overcome natural resistance mechanisms? • it includes the low catalase producers of Wayne, and almost all the AccuProbe-1-negative strains
Conclusions • A more precise definition of various M. kansasiiisolates would provide significant contribution to understanding of its biological and epidemiological key aspects • An international task force, including microbiologists, epidemiologists and clinicians, is needed to efficiently take up the challenge of M. kansasii