Download

1 / 31
310 likes | 321 Views
Nuovi inibitori irreversibili di EGFR. Cesare Gridelli Division of Medical Oncology “S.G. Moscati” Hospital – Avellino (Italy) cgridelli@libero.it. NEGATIVE TRIAL. 1. N= 440 patients. Stratification -Race -Exon 19 v 21.

E N D
Nuovi inibitori irreversibili di EGFR Cesare Gridelli Division of Medical Oncology“S.G. Moscati” Hospital – Avellino (Italy)cgridelli@libero.it
NEGATIVE TRIAL 1 N= 440 patients Stratification -Race -Exon 19 v 21
Comparison of the Efficacy of Dacomitinib v Erlotinib for NSCLC Pts with Del 19/21 121 EGFR Mutant Patients Retrospectively analysed from ARCHER 1028 (Ramalingam S JCO 2012) and ARCHER 1009 (Ramalingam S Lancet Oncol 2014) OS PFS Ramalingam SS et al. WCLC 2015
ARCHER 1050: Randomized Phase III Study DacomitinibvsGefitinib Dacomitinib 45mg qd RANDOMIZE • Advanced NSCLC • Adenocarcinoma • EGFR exon 19/21 mut+ • First-line treatment • PS 0-1 Primary endpoint in PFS 14.8 vs 9.5 months 1 Gefitinib 250mg qd 1 N= 440 patients Stratification -Race -Exon 19 v 21
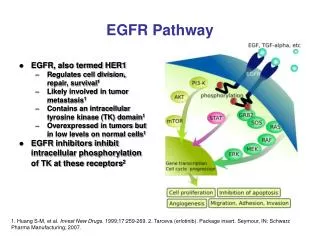
Acquired resistance in EGFR Mut+ NSCLC Mechanisms of acquired resistance to EGFR TKIs • Acquired resistance to EGFR TKIs in metastatic setting is inevitable • The average PFS is 8–13 months Activation of other receptor tyrosine kinases? (eg. ERBB2 amplification) FAS/NFB activation? Epithelial-mesenchymal transition?(AXL, Slug activation?) Loss or spliced variant of BIM? Other? (eg. CRKL or ERK amplification) ~30–40% ~60% second-site EGFR mutations (mostly T790M) ~1% BRAF mutations ~5% small-cell cancer transformations ~5% PIK3CA mutations -5–10% MET amplification Ohashi et al, J Clin Oncol 2013
Adequacy and Complications of re-biopsy • 126 patients referred for repeat biopsy • with NSCLC resistant to conventional chemotherapy or EGFR Tki • 94 patients (31 men, 63 women) selected for rebiopsy (75%) • (25% of case it was not possible) • Technical success rate for biopsy was 100% (80% suitable for mutational analyses). • Postprocedural complications occurred in 13 (14%) patients Yoon HJ et al, Radiology 2012
3rd Generation Irreversible EGFR TKIs Under Development: AZD9291 • Selectively targets mutated EGFR, including T790M • Phase I dose escalation study in patients with EGFR Mut+ disease and PD on EGFR TKI • Encouraging activity : • 61 % response rate months in 127 pts T790M+ • 21 % response rate in 61 pts T790M- • No DLTs • Recommended dose: 80 mg daily Janne et al. N Engl J Med 2015; 372: 1689–1699
FLAURA ZD9291: clinical development • Phase III – efficacy and safety of AZD9291 vs gefitinib or erlotinib in first-line patients with EGFR M+, advanced/metastatic NSCLC
AURA2: Phase II, open-label, single-arm study Primary objective To investigate the efficacy of AZD9291 by assessment of ORR (RECIST 1.1 BICR) Patients with confirmed EGFRm locally advanced or metastatic NSCLC who have progressed following prior therapy with an approved EGFR-TKI • Key inclusion criteria • Aged ≥18 (≥20 in Japan) • Confirmation of tumor EGFR mutation associated with EGFR-TKI • At least one lesion suitable for accurate repeated measurements • WHO performance status 0 or 1 • Acceptable organ function • Stable brain metastases allowed Central T790M mutation testing* of biopsy sample collected following confirmed disease progression T790M positive (n=210) AZD9291 80 mg once daily T790M negative Not eligible for enrollment *The EGFR T790M mutation status of the patient’s tumor was prospectively determined by the designated central laboratory using the cobas™ EGFR Mutation Test (Roche Molecular Systems) by biopsy taken after confirmation of disease progression on the most recent treatment regimen BICR, blinded independent central review; EGFR, epidermal growth factor receptor; EGFRm, EGFR-TKI-sensitizing mutation; NSCLC, non-small cell lung cancer; ORR, objective response rate; RECIST, Response Evaluation Criteria In Solid Tumors; TKI, tyrosine kinase inhibitor; WHO, World Health Organization
Tumor response (independent central review) 100 80 Best percentage change from baseline in target lesion – all patients 60 40 20 0 -20 Complete response Partial response Stable disease Progressive disease Not evaluable -40 -60 -80 -100 Mitsudomi T et al. WCLC 2015
Duration of response and progression-free survival 1.0 1.0 Duration of response Progression-free survival 0.9 0.9 0.8 0.8 0.7 0.7 0.6 0.6 Probability of progression-free survival 0.5 Probability of response 0.5 0.4 0.4 0.3 0.3 0.2 Censored observations 0.2 AZD9291 80 mg Censored observations 0.1 AZD9291 80 mg 0.1 0.0 0.0 0 3 6 9 12 0 3 6 9 12 Number of patients at risk: Month Number of patients at month: Month 210 172 115 15 141 123 43 Mitsudomi T et al. WCLC 2015
AURA 3 TRIAL: AZD9291 vsChemotherapy in II line in patients with EGFR activating mutation and T790M+ AZD9291 (80 mg daily) RANDOMIZE • Advanced NSCLC • Adenocarcinoma • EGFR mut+ • EGFR T790M+ • Second-line treatment • PS 0-1 1 Chemotherapy CDDP+Alimta 1
ZD9291 in 1-line EGFR M+ (19/21): Response in first-line cohorts by dose D 100 90 Best percentage change in target lesion size – all patients 80 D 70 D D 60 D D D 50 D 40 D D 30 20 D 10 0 -10 -20 -30 D -40 D -50 -60 D -70 80 mg D -80 D -90 160 mg -100 Ramalingam S et al. WCLC 2015
DoR and PFS in AZD9291 first-line cohorts (investigator assessed) Duration of response Progression-free survival 1.0 1.0 0.9 0.9 0.8 0.8 0.7 0.7 0.6 0.6 Probability of response 0.5 Probability of response 0.5 0.4 0.4 0.3 0.3 0.2 0.2 AZD9291 80 mg Censored observation AZD9291 80 mg Censored observation 0.1 0.1 AZD9291 160 mg Censored observation AZD9291 160 mg Censored observation 0.0 0.0 0 3 6 9 12 15 18 0 3 6 9 12 15 18 Number of patients at risk: Number of patients at month: Month Month 3 22 19 12 80 mg 30 26 23 0 14 10 5 20 20 17 80 mg 0 23 17 0 160 mg 30 29 27 0 18 8 0 25 25 21 160 mg Ramalingam S et al. WCLC 2015
FLAURA Phase III trial: AZD9291 vs Gefitnib or Erlotinib in I line in patients with EGFR mutation AZD9291 (80 mg daily) RANDOMIZE • Advanced NSCLC • Adenocarcinoma • EGFR mut+ • First-line treatment • PS 0-1 1 1 Gefitinib or Erlotinib
3 rd generation EGFR TKIs under development: Rociletinib (CO-1686) • Selectively targets mutated EGFR,including T790M • spares EGFR WT • Phase I dose escalation study in EGFRMut+ T790M+(n=243/458) • encouraging activity: • 53% response rate • Median PFS 8 months • AE profile consistent with lack of EGFR WT inhibition • T790M negative 37% OR • Positive agreement T790M liquid (81%) vs tissue (87%) biopsy • Recommended dose: 1000 mg • (500 mg BID ) Sequist L et al, ASCO 2015
Dose Optimization of Rociletinib for T790M Mutated NSCLC 100 80 60 40 20 0 −20 −40 −60 −80 −100 SLD change from baseline (%) + Ongoing Grade ≥3 treatment-related AEs observed in >10% of patients, n (%) The risk-benefit profile of rociletinib is optimal at the recommended dose (500 mg BID) 500mg BID HBr 625mg BID HBr 750mg BID HBr Goldman JW et al. WCLC 2015
TIGER-X: Phase 1/2 study of rociletinib in advanced NSCLC • ORR in centrally confirmed tissue T790M-positive pts (n=48) enrolled at the 500mg BID dosing level was 60% • ORR in centrally confirmed tissue T790M-negative pts (n=35) was 37%1 • Updated results in centrally confirmed tissue T790M-negative pts are presented • As of August 11, 2015, 111 and 482 pts (T790M±) were enrolled on the phase 1 and 2 portions, respectively Phase 1 (Dose Escalation) Phase 2 Expansion Cohorts (Required Central Tissue T790M Testing) Rociletinib Treatment (free base rociletinib, followed by 500, 625, 750, and 1000mg BID HBr) • Key outcome measures • Safety • Tolerability • PK profile • ORR 2nd-line patients PD upon 1 immediate prior TKI 500mg BID 625mg BID 21-day cycles; escalate to MTD >2nd-line patients PD upon ≥2 TKI or chemotherapy 750mg BID Wakelee H et al, WCLC 2015
Why do T790M-negative pts respond to rociletinib? • Qiagen therascreen and cobas central T790M tests are highly concordant • A sample that tests negative by one central test likely to be negative by other • Tumor heterogeneity • Not all cells express T790M; tissue biopsy samples one small area • Plasma test may be more representative, especially with extrathoracic spread • Other mechanisms of rociletinib action may be important • Rociletinib inhibits IGF-1R and IR kinases • IGF-1R/IR may drive resistance to initial EGFR inhibitor therapy • In a preclinical study, treatment with a T790M-potent EGFR TKI prevented emergence of the EGFR T790M mutation, resulting in sequential acquisition of non-T790M resistance mechanisms involving IGF-1R and MAPK pathways1 Wakelee H et al, WCLC 2015 1. Cortot A, et al. Cancer Res. 2013;73:834-43.
Trials enrolling in 2014 TIGER4 (phase 2) (TIGER2like ;pts T790M plasma)
TIGER 1 PHASE II TRIAL: 1-line Rociletinibvs Erlotinib in patients with EGFR mutation Rociletinib RANDOMIZE • Advanced NSCLC • Adenocarcinoma • EGFR mut+ • First-line treatment • PS 0-1 1250 mg (625 mg BID) 1 Erlotinib 1
TIGER 3 TRIAL: Rociletinib vs chemotherapy in pretreated patients with EGFR mutation and T790M+/- RANDOMIZE Rocilietinib • Advanced NSCLC • Adenocarcinoma • EGFR mut+ • EGFR T790M+ or - • Third or more line treatment • PS 0-1 1250 mg (625 mg BID) 1 Single agent Chemotherapy (Pem/Gem/Txt/Tax) 1
Study Design Recommended dose: 800 mg (400 mg BID)
HM61713 Best Overall Response: Expansion Part
Progression-Free Survival<br />: Expansion part (T790M+ versus T790M-)
HM61713 PHASE II TRIAL in 2-line for patients with EGFR activating mutation and T790M+ • Advanced NSCLC • Adenocarcinoma • EGFR mut+ • EGFR T790M+ • Second-line treatment (previous TKI) • PS 0-1 HM61713 800 mg (400 mg BID)
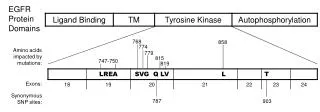
NATURE MEDICINE | BRIEF COMMUNICATION Acquired EGFR C797S mutation mediates resistance to AZD9291 in non–small cell lung cancer harboring EGFR T790M Kenneth S Thress, Cloud P Paweletz, Enriqueta Felip, Byoung Chul Cho, Daniel Stetson, Brian Dougherty, Zhongwu Lai, Aleksandra Markovets, Ana Vivancos, Yanan Kuang, Dalia Ercan, Sarah E Matthews, Mireille Cantarini, J Carl Barrett, Pasi A Jänne & Geoffrey R Oxnard Nature Medicine21, 560–562 (2015) T790M+ C797S+ 6 pts MOLECULAR SUBTYPES OF RESISTANCE AZD9291 Resistance T790M+ C797S- T790M+ 5 pts 15 pts T790M- C797S- Del19+ or Mut21+ 4 pts • Cell-free plasma DNA (cfDNA) • Firstly next-generation sequencing of cfDNA from 7 patients detecting an acquired EGFR C797S mutation in 1 patient • Then droplet digital PCR on serial cfDNA specimens collected from 15 AZD9291-treated patients • All positive for the T790M mutation before treatment, but after AZD9291 resistance: • 6 cases acquired the C797S mutation • 5 cases maintained the T790M mutation but did not acquire the C797S mutation • 4 cases lost the T790M mutation despite the presence of the underlying EGFR activating mutation
Mechanisms of Acquired Resistance to AZD9291 in EGFR T790M Positive Lung Cancer • 15 (22%) out of 67 patients, had detectable C797S, all with detectable T790M (T790+/C797S+) • C797S was more common with EGFR exon 19 del (13/43, 30%) vs those with L858R (2/24, 8%, p=0.06) • 32 of 67 (48%) had no detectable T790M in plasma despite presence of the EGFR-TKI-sensitizing mutation, suggesting overgrowth of an alternate resistance mechanism, such as MET or HER2 amplification or BRAF V600E Oxnard G et al. WCLC 2015