Download
1 / 12
150 likes | 502 Views
Head Injury. Practical Aspects of Management and Transfer. Susanne Young. CONTENT. Head Injuries Background INITIAL MANAGEMENT Current Guidelines- ATLS Prevention of secondary Brain Injury (1-4) Use of adjunct therapies TRANSFER Which Sedative? AAGBI. BACKGROUND.

E N D
Head Injury Practical Aspects of Management and Transfer. Susanne Young
CONTENT • Head Injuries Background • INITIAL MANAGEMENT • Current Guidelines- ATLS • Prevention of secondary Brain Injury (1-4) • Use of adjunct therapies • TRANSFER • Which Sedative? • AAGBI
BACKGROUND • Head injury accounts for approximately 300 per 100 000 hospital admissions per year; of these, 9 per 100 000 die. • RTA's account for about 25% of cases and about 60% of deaths; many die before reaching hospital. • The aim of management is to minimise damage arising from secondary complications.
PROGNOSIS • Traumatic Brain Injury- prognosis at 48HRS GCS <8- severe 9-12- moderate 13-15- mild
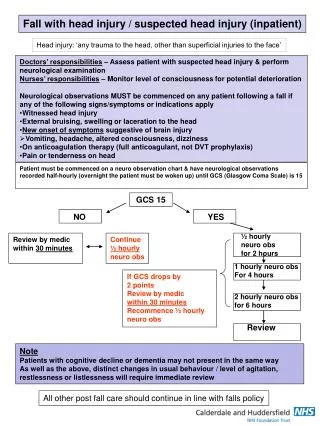
INITIAL MANAGEMENT • A-secure a clear airway and control cervical spine • B-treat hypoventilation, severe chest injury • C-control haemorhage and treat shock • D-assess disability • E-exposure, prevent hypothermia *
Principles of management • Prevention of secondary cerebral injury: • 1 Hypoxia • 2 ICP • 3 CPP and CBF • 4 Cerebral metabolism
1 HYPOXIA • PO2 <10kPa for any reason • If hard collar Consider: • 2 person Manual in-line immobilisation • 3rd person cricoid • Use of McCoy blade • ?Blind Nasotracheal intubation –exc if Basal skull #- if skilled
2 Control of ICP • Signs of raised ICP (>20mmHg) Papilloedema, BP , HR ,fixed pupils, flaccid, irreg resps (brainstem involvement) • ?Hypoventilate- if in doubt DON’T Moderate hypocapnia CO2 3.5-4 OK Consider if GCS drops suddenly Very low CO2 –vasoconstriction ischaemia
Control of ICP (contd). • Fluid balance- overload can exacerbate cerebral and pulmonary oedema • Sedate initially- Propofol first line Add Midaz if ineffective ? Thio- may cause haemodynamic disturbance • ? Mannitol 0.25-1g/kg (100ml 20%). Buys time only, nephrotoxic- watch uo.
3 Control of CPP and CBF • CPP= MAP- ICP mmHg • Min CPP 60/70 for adequate perfusion • Cushing reflex designed to restore CPP in presence of ICP therefore • Don’t treat Hypertension! • Mainstay of treatment is to keep SBP>90 • Steroids ineffective (palliative care only)
Control of Cerebral Metabolism • Prevent fits. Prophylaxis in first week. • Phenytoin 15mg/kg loading • Avoid Benzo’s if poss. • ? Active cooling Moderate hypothermia (32-33 for 24hrs) of benefit if GCS at presentation5-7
TRANSFER • INTUBATE AND VENTILATE- but don’t hyperventilate. • SEDATE WITH PROPOFOL • A LINE, CATHETER, ECG etc • Prophylactically- join AAGBI! • become a member of the Group of Anaesthetists in Training (GAT). • Free insurance to cover you during any inter-hospital ambulance transfers !