Download
1 / 55
550 likes | 666 Views
A STUDY OF AVIAN INFLUENZA (H5N1) INFECTION IN EGYPTIAN CHILDREN. By Dr. Nasser Abdou Kolkailah MD pediatrics, Benha University Ministry Of health consultant of Avian Influenza in pediatrics. E-mail: nasserkolkailah@yahoo.com.

E N D
A STUDY OF AVIAN INFLUENZA (H5N1) INFECTION IN EGYPTIAN CHILDREN By Dr. Nasser Abdou Kolkailah MD pediatrics, Benha University Ministry Of health consultant of Avian Influenza in pediatrics. E-mail: nasserkolkailah@yahoo.com
“When you want something, all the universe conspires in helping you to achieve it.” Paulo Coelho The Alchemist
Avian Influenza • Recent cluster of severe infection with Avian Influenza virus was first documented in Hong Kong in 1997.
The global number of H5N1 cases is 554; out of whom 324 died. • Egypt confirmed the 1st case of H5N1 virus in its domestic poultry on February 17th , 2006 and the 1st human case on March 17th , 2006. Since then, there have been 144 cases, among whom 48 died.
This can be explained by the fact that young children often treat poultry as pets. Children often care for domestic poultry by feeding them, cleaning pans and gathering eggs.
In children, sex predominance has not been noted. In adults, females have been more infected (54 cases) than males (17 cases) with a P value of < 0.01, which is statistically highly significant and reassures that those backyards still remain the main source of infection.
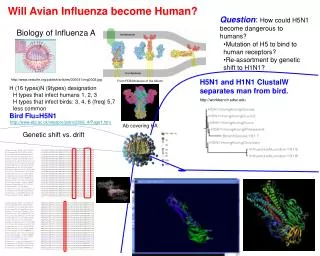
Figure:3 Annual distribution of human avian influenza cases by age group in Egypt
This may be attributed to the efforts exerted by the Egyptian Ministry of Health in controlling farms as a main source of infection in adults. Nevertheless, there are difficulties faced in combating backyards which represent the main source of infection in children who play with apparently healthy poultry during the early infectivity period. • Another assumption is the possibility of sub clinical infection in adults.
In 2010 & 2011 the rates were reversed. • This may be due to failure of the ministry of health and ministry of agriculture in limiting the trading of live poultry.
Figure 4: Seasonal predilection of H5N1 human infection in Egypt:
Figure 5: Worldwide seasonal predilection of H5N1 human infection
All cases had an obvious history of close contact with infected poultry. There have been 2 affected sibs and 2 affected cousins. The exposure to a common source of infection is rather a stronger explanation than human to human transmission. • The duration between the exposure to dead birds and the appearance of symptoms ranged from 3 to 10 days.
Clinical Data: • 49 cases presented with symptoms and signs of upper respiratory catarrh and they were stable. • 10 cases presented with dyspnea grade II and clinical examination revealed acute bronchitis. • 14 cases were suffering from severe bronchopneumonia; hepatomegaly was a finding in 5 of them.
Laboratory results: • RT- PCR confirmed the diagnosis of H5N1 infection in all cases. • Our results have shown anemia in 20 cases, leucopenia in 14, lymphopenia in 7 and thrombocytopenia in 10. • There have been 8 cases that developed secondary bacterial infection proved by leucocytosis, rising titre of CRP, while blood culture was + ve in 3 cases. • Mild elevation of liver enzymes has been noted in 12 cases and mild elevation of serum creatinine in 6.
Radiological Findings: • Increased bronchovascular markings in 10 cases denoting acute bronchitis. • Bronchopneumonia was found in 14 cases (figures 5-10). • CT scan was requested for 2 cases of pneumonia (figures 11-12).
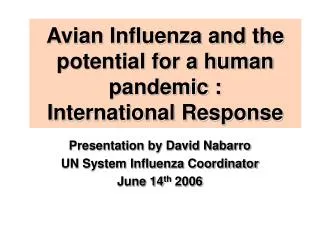
Figure 12 A: Chest CT scans of case number 18: 22/6/2007: Sizable areas of pneumonic consolidation process seen at right middle lobe and left basal lower segments, with fine air broncogram at site. The left basal segment pneumonic area showed small +1 cm cavity for follow up, left basal pleuro-pulmonary reaction, patent main tracheo-bronchial tree, fine left basal atelectatic bands, and no evidence of hilar masses or mediastinal lymphadenopathy
Figure 12 B: Chest CT scans of case number 18: 22/7/2007: Improvement of the consolidative process previously noted at both lower lobes mainly affecting the apical and anterior basal segment of right lower lobe and the posterior and anteromedial basal segments of the left lower lobe.
Figure 12 C: Chest CT scans of case number 18: 21/8/2007: Regression of the previously noted bilateral lower lobe subsegmental air space consolidation changes with areas of ground glass opacities are still noticed
Figure 13: Chest CT scans of case number 28: Multiple areas of pneumonic patches of chest infection. Segmental collapse area of right middle lobe. Areas of fine basal atelectatic bands.
Our management plan is to eradicate the virus and to prevent and treat body systems dysfunction. • Tamiflu has been given to all cases according to the standard dose regimen. • The start of Tamiflu ranged from the 1st day to the 6th day after the onset of symptoms. • One case started therapy 2 weeks after the onset of symptoms due to a delayed etiological diagnosis. • Course of therapy ranged from 5 to 33 days.
In addition to the standard therapy of Tamiflu, 10 cases received polyclonal IVIG • 7 cases received it on the 1st day of admission as they suffered from severe bronchopneumonia. • The 8th and 9th cases were stable and received polyclonal IVIG due to persistent positive cultures after Tamiflu therapy. • The 10th case developed respiratory failure as a complication of pneumonia and received polyclonal IVIG two weeks after the onset of symptoms due to delayed etiological diagnosis.
All cases have shown progressive improvement except 7 pneumonic cases. • The 1st case deteriorated clinically and developed circulatory collapse which was treated by inotropics (Dopamine) and has fully recovered. • The 2nd case deteriorated clinically and developed cardio respiratory failure and was mechanically ventilated for four days and has eventually recovered.
The 3rd case was mechanically ventilated as he developed respiratory failure and ARDS, but unfortunately died. • 4 cases have developed respiratory failure and died before being referred to our center.
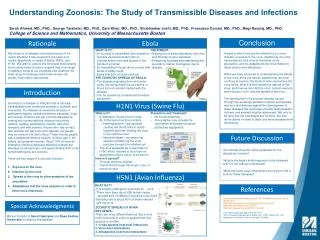
Figure 14: Human Avian Influenza (H5N1) cases by age group and outcome in Egypt (May 2011)
Why clinical course and outcome among Egyptian children were better compared to other countries? 1- Early suspicion of Avian Influenza. 2- Meticulous prevention of secondary bacterial infection. 3- Administration of polyclonal IVIG in severe cases.
The possibility of unresponsiveness to Tamiflu as it was started 5 days after the onset of symptoms. My considerations of adding polyclonal IVIG to the standard therapy regimen in the 1st case
Apoptosis may play a major role in the pathogenesis of influenza (H5N1) virus in humans by destroying alveolar epithelial cells. Whether apoptosis is a direct result of the viral replication or a consequence of an over activation of the immune system (cytokine storm) has not been clearly elucidated. Polyclonal IVIG has proved to have a dual action. It functions as an antiviral therapy neutralizing the virus and immunomodulating agent suppressing various inflammatory mediators; including cytokines, chemokines, and metalloproteinases.
The evidence of polyclonal IVIG being greatly effective in recovery: • The case has been purely viral with no secondary bacterial infection, Thus the antibiotics given were not the reason for recovery.
The role of Tamiflu is doubtful due to: a. The therapy started 5 days after the onset of symptoms, which was rather late. b. The severe systemic hypoperfusion could affect the intestinal absorption of the drug.
The case developed life threatening pneumonia denoting her immunodeficient state. Thus her innate immunity was not the key for recovery.
Due to all the facts mentioned before, we started polyclonal IVIG for six severe cases with bronchopneumonia on the first day of therapy and they fully recovered.
More evidence supporting the effectiveness of polyclonal IVIG: • An eight-year-old boy received Tamiflu for 5 days before being referred to the designed hospital in an advanced stage of severe bronchopneumonia and huge hepatomegaly. He was given IVIG for 5 days as an adjuvant therapy, which resulted in full recovery after 5 days.
Four stable cases among the 2009 cluster and one case in the 2011 cluster, showed a delayed sero-conversion for more than 20 days and received Tamiflu only. On the contrary, the use of Polyclonal IVIG as an adjuvant therapy in three critical cases of severe bronchopneumonia and respiratory failure achieved both a good clinical response and a complete eradication of the virus in less than 10 days.
Conclusion: • Backyards represent the major source of infection in Egypt. Thus, H5N1 infection targets mainly young children and housewives.
There is a seasonal predilection of H5N1 in both winter and early spring .
No evidence has supported human to human transmission till now.
The early seeking of medical advice represents an important contribution to a better prognosis in children.