Download
1 / 119
1.19k likes | 2.03k Views
Pathology of arthritis for medical students.

E N D
Pathology of Arthritis “ Never let the competition define you. Instead, you have to define yourself based on a point of view you care deeply about.” – Tom Chappel
CPC 3.7 - Rheumatology <ul><li>“ I have very bad joint pain” </li></ul><ul><ul><li>Scenario 1: Ms F.M. 19 year old student </li></ul></ul><ul><ul><li>Scenario 2: Mr J.W. 52 year old publican </li></ul></ul><ul><ul><li>Scenario 3: Mrs N. 69y retired Sports teacher. </li></ul></ul><ul><li>Notes to Tutors: </li></ul><ul><ul><li>Discuss DD - variety of clinical scenarios. </li></ul></ul><ul><ul><li>Remember/revise serious causes of acute joint pain esp. septic arthritis and rheumatic fever (revise Jones criteria). </li></ul></ul><ul><ul><li>Differentials to include fibromyalgia, polymyalgia rheumatica, SLE etc. </li></ul></ul>Rheumatoid A. Gouty Arthritis. Osteoarthritis. CPC 3.7 - Rheumatology <ul><li>“ I have very bad joint pain” </li></ul><ul><ul><li>Scenario 1: Ms F.M. 19 year old student </li></ul></ul><ul><ul><li>Scenario 2: Mr J.W. 52 year old publican </li></ul></ul><ul><ul><li>Scenario 3: Mrs N. 69y retired Sports teacher. </li></ul></ul><ul><li>Notes to Tutors: </li></ul><ul><ul><li>Discuss DD - variety of clinical scenarios. </li></ul></ul><ul><ul><li>Remember/revise serious causes of acute joint pain esp. septic arthritis and rheumatic fever (revise Jones criteria). </li></ul></ul><ul><ul><li>Differentials to include fibromyalgia, polymyalgia rheumatica, SLE etc. </li></ul></ul>Rheumatoid A. Gouty Arthritis. Osteoarthritis.
Signs/Symp. & Pathogenesis <ul><li>Pain, fever </li></ul><ul><li>Swelling </li></ul><ul><li>Limited mobility </li></ul><ul><li>Deformity </li></ul><ul><li>High ESR </li></ul><ul><li>Lymphadenopathy </li></ul><ul><li>Fractures </li></ul><ul><li>Infl. Capsule & Syn. </li></ul><ul><li>Synovial effusion. </li></ul><ul><li>Fusion- Fibrosis, bony </li></ul><ul><li>Cartilage damage. </li></ul><ul><li>Inflam. Mediators –AI </li></ul><ul><li>Chronic inflam - T cell </li></ul><ul><li>Osteoporosis. </li></ul> Signs/Symp. & Pathogenesis <ul><li>Pain, fever </li></ul><ul><li>Swelling </li></ul><ul><li>Limited mobility </li></ul><ul><li>Deformity </li></ul><ul><li>High ESR </li></ul><ul><li>Lymphadenopathy </li></ul><ul><li>Fractures </li></ul><ul><li>Infl. Capsule & Syn. </li></ul><ul><li>Synovial effusion. </li></ul><ul><li>Fusion- Fibrosis, bony </li></ul><ul><li>Cartilage damage. </li></ul><ul><li>Inflam. Mediators –AI </li></ul><ul><li>Chronic inflam - T cell </li></ul><ul><li>Osteoporosis. </li></ul>
"Thinking is progress. Non-thinking is stagnation of the individual, organisation and the country. Thinking leads to right action. Knowledge without action is useless and irrelevant. Knowledge with action, converts adversity into prosperity.” - - APJ Abdul Kalam, President of India. "Thinking is progress. Non-thinking is stagnation of the individual, organisation and the country. Thinking leads to right action. Knowledge without action is useless and irrelevant. Knowledge with action, converts adversity into prosperity.” - - APJ Abdul Kalam, President of India.
Pathology of Arthritis Dr. Venkatesh M. Shashidhar. Associate Professor & Head of Pathology Pathology of Arthritis Dr. Venkatesh M. Shashidhar. Associate Professor & Head of Pathology
Joints: Anatomy & Physiology <ul><li>Mobility - Cranial sutures Shoulder joint. </li></ul><ul><li>Articular cartilage – hyaline – friction res. </li></ul><ul><li>Synovial fluid – lubric/nutri, Type A & B synoviocytes. Hyaluronidase </li></ul><ul><li>Continuous production and absorption. Affected by Inflammation, immobility. </li></ul><ul><li>Capsule, ligaments, menisci. </li></ul><ul><li>Vascular, rich nerve supply </li></ul><ul><li>Art. Cartilage * </li></ul> Joints: Anatomy & Physiology <ul><li>Mobility - Cranial sutures Shoulder joint. </li></ul><ul><li>Articular cartilage – hyaline – friction res. </li></ul><ul><li>Synovial fluid – lubric/nutri, Type A & B synoviocytes. Hyaluronidase </li></ul><ul><li>Continuous production and absorption. Affected by Inflammation, immobility. </li></ul><ul><li>Capsule, ligaments, menisci. </li></ul><ul><li>Vascular, rich nerve supply </li></ul><ul><li>Art. Cartilage * </li></ul>
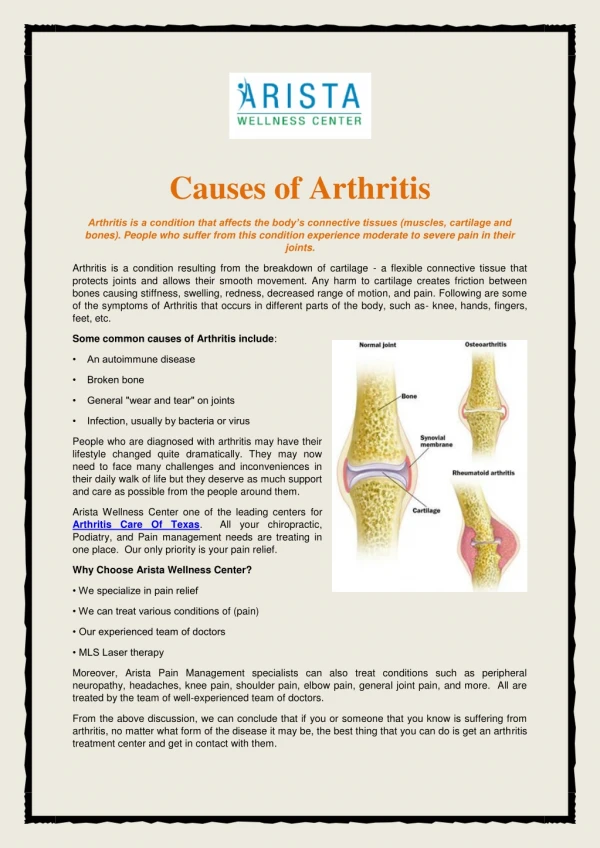
Arthritis - Introduction <ul><li>Joints: Use it or Loose it….! </li></ul><ul><li>Inflammatory & Degenerative . </li></ul><ul><li>Inflammation - Common </li></ul><ul><ul><li>Trauma, Infections & Autoimmune . </li></ul></ul><ul><ul><li>Autoimmune injury (& Heart valves) </li></ul></ul><ul><ul><li>Damage Exposure of hidden antigens. </li></ul></ul><ul><li>Degeneration – wear & tear – Age / Stress / disease / life style </li></ul> Arthritis - Introduction <ul><li>Joints: Use it or Loose it….! </li></ul><ul><li>Inflammatory & Degenerative . </li></ul><ul><li>Inflammation - Common </li></ul><ul><ul><li>Trauma, Infections & Autoimmune . </li></ul></ul><ul><ul><li>Autoimmune injury (& Heart valves) </li></ul></ul><ul><ul><li>Damage Exposure of hidden antigens. </li></ul></ul><ul><li>Degeneration – wear & tear – Age / Stress / disease / life style </li></ul>
Arthritis – Clinical features: <ul><li>Pain </li></ul><ul><ul><li>Inflammation - capsule, synovium, periosteum. </li></ul></ul><ul><li>Swelling: </li></ul><ul><ul><li>inflammation, effusion, proliferation. </li></ul></ul><ul><li>Restricted movement </li></ul><ul><ul><li>pain, fluid, synovial swelling, damage. </li></ul></ul><ul><li>Deformity </li></ul><ul><ul><li>mal-alignment, erosion, ankylosis </li></ul></ul> Arthritis – Clinical features: <ul><li>Pain </li></ul><ul><ul><li>Inflammation - capsule, synovium, periosteum. </li></ul></ul><ul><li>Swelling: </li></ul><ul><ul><li>inflammation, effusion, proliferation. </li></ul></ul><ul><li>Restricted movement </li></ul><ul><ul><li>pain, fluid, synovial swelling, damage. </li></ul></ul><ul><li>Deformity </li></ul><ul><ul><li>mal-alignment, erosion, ankylosis </li></ul></ul>
. Arthritis Clinical Classification: <ul><li>Monoarthritis: </li></ul><ul><ul><li>Local, asymmetric, secondary. </li></ul></ul><ul><ul><li>Acute: Bacterial , Trauma , Crystal, Reactive </li></ul></ul><ul><ul><li>Chronic :Tuberculosis, Lyme, Fungal, Trauma, Tumors. </li></ul></ul><ul><li>Polyarthritis: </li></ul><ul><ul><li>Chronic, symmetric, systemic. </li></ul></ul><ul><ul><li>Autoimmune , degenerative , Crystal . </li></ul></ul><ul><ul><li>Rarely infective. </li></ul></ul>
. Polyarthritis Classification: <ul><li>Autoimmune: </li></ul><ul><ul><li>Rheumatic, Rheumatoid, Ankylosing spondylitis, Reiter syndrome etc. </li></ul></ul><ul><li>Degenerative : Osteroarthritis </li></ul><ul><li>Crystal Deposition : </li></ul><ul><ul><li>Gout – Monosodium urate </li></ul></ul><ul><ul><li>CPPD - Pseudo Gout </li></ul></ul><ul><li>Infective - Septic , TB, Lyme etc. rare. </li></ul>
. Epidemiology of RA <ul><li>Prevalence - ~ 1% of US population </li></ul><ul><li>Female : Male ratio = 2:1 </li></ul><ul><li>Strong association with HLA DR4. </li></ul><ul><li>Concordance in identical twins only 30%. </li></ul><ul><li>Genetic + Environmental + Autoimmune </li></ul>
. RA - Definition: <ul><li>Chronic </li></ul><ul><li>Multisystem </li></ul><ul><li>autoimmune </li></ul><ul><li>inflammatory disorder primarily affecting joints producing a proliferative synovitis that often progresses to destruction of the articular cartilage and ankylosis. </li></ul>
. Etiology : <ul><li>Genetic Susceptibility: </li></ul><ul><ul><li>HLA DR4, or DR1 in 65% to 80% cases. </li></ul></ul><ul><li>Microbial inciting agent: </li></ul><ul><ul><li>Epstein-Barr virus, Borrelia & Mycoplasma..? </li></ul></ul><ul><li>Autoimmunity: </li></ul><ul><ul><li>IGM anti IgG – RA Factor. </li></ul></ul><ul><ul><li>Helper T cell (CD4) against type II collagen & cartilage glycoprotein-39 </li></ul></ul>
. Immuno-dysregulation in RA <ul><li>T lymphocytes type II collagen & superantigen releasing cytokines inflammation. </li></ul><ul><li>B cells IgM Rheumatoid factor – anti IgG. </li></ul><ul><li>Macrophages surround RF factor complex type III injury (immune complex) cytokine release inflammation damage. </li></ul>
. Morphology - Synovitis : <ul><li>Proliferative synovitis with lymphocytes (CD4), plasma cell & macrophages Pannus . </li></ul><ul><li>Organizing fibrin ( rice bodies ). </li></ul><ul><li>Neutrophils on the joint surface and fluid. </li></ul><ul><li>Juxta-articular erosions, cysts & osteoporosis </li></ul><ul><li>Fibrous ankylosis . </li></ul><ul><li>Skin - Rheumatoid nodules </li></ul><ul><li>Vasculitis (commonly of digital arteries) </li></ul>
. RA - Clinical Features: <ul><li>Morning stiffness . </li></ul><ul><li>Arthritis in 3 or more joint areas. </li></ul><ul><li>Arthritis of small hand joints. </li></ul><ul><li>Symmetric arthritis. </li></ul><ul><li>Rheumatoid nodules . </li></ul><ul><li>Serum rheumatoid factor . </li></ul><ul><li>Typical radiographic changes </li></ul>At least 4 features for diagnosis.
. Extra-Articular RA <ul><li>Rheumatoid Nodules. </li></ul><ul><li>Vasculitis. </li></ul><ul><li>Pleuritis. </li></ul><ul><li>Pericarditis. </li></ul><ul><li>Tendonitis. </li></ul><ul><li>Fibrosing alveolitis. </li></ul>
. Rheumatoid Nodule (skin): Palisading Macrophages Central Fibrinoid Necrosis
. Degenerative - Inflammatory <ul><li>Both sexes equal. </li></ul><ul><li>Pain through the day </li></ul><ul><li>No morning stiffness. </li></ul><ul><li>Stiffness, less pain. </li></ul><ul><li>Bony swelling. </li></ul><ul><li>No soft tissue swelling </li></ul><ul><li>Uni/Bilateral, Asymmetrical. </li></ul><ul><li>Females more. </li></ul><ul><li>Morning stiffness >1h. </li></ul><ul><li>Less with movement. </li></ul><ul><li>Pain & redness </li></ul><ul><li>Inflammation & swelling of soft tissue. </li></ul><ul><li>Late bone swelling. </li></ul><ul><li>Bilateral, Symmetrical. </li></ul>
. RA Joint destruction, ankylosis: Subluxation deformities and severe osteopenia in chronic rheumatoid arthritis treated with corticosteroids
. RA Muscle wasting. Polyarthritis and muscle atrophy in chronic juvenile rheumatoid arthritis.
. Osteoarthritis Degenerative arthr osis . (Osteoarthrosis)
. Osteoarthritis: <ul><li>Degenerative end result - (ageing) >80% in >65y . (20% clinically significant) </li></ul><ul><li>Progressive erosion & fibrillation of articular cartilage forms Loose bodies. </li></ul><ul><li>Large weight bearing joints. </li></ul><ul><li>Hardened articular bone – eburnation. & Subarticular cyst formation in bone. </li></ul><ul><li>Periarticular osteophyte formation. </li></ul><ul><li>Mild inflammation but painful, morning stiffness. </li></ul><ul><li>Limited range of movements - Heberden nodes. </li></ul>
. Normal -- Femur Head -- OA Normal Osteoarthritis
. Osteoarthritis: 1- Eburnation of bone 2- Subchondral cyst 3- Residual cartilage
. OA: Ebernation & Osteophytes Exposed bone Osteophytes
. Femur Osteroarthritis: Bone exposure Cartilage degeneration
. Radiologic Features: <ul><li>nonuniform joint space loss, </li></ul><ul><li>osteophyte formation, </li></ul><ul><li>cyst formation </li></ul><ul><li>subchondral sclerosis </li></ul><ul><li>Sclerosis, ankylosis & deformity. </li></ul>
. Osteoarthritis: <ul><li>Narrow joint space </li></ul><ul><li>Lipping – osteophyte </li></ul><ul><li>Dislocation </li></ul><ul><li>Osteoporosis. </li></ul>