Download
1 / 78
810 likes | 2.36k Views
Pathology of Meningitis, CNS infections, increased cerebral pressure, brain herniations etc. for pre clinical medical students.

E N D
Pathology of Meningitis & CNS infections. Applied Faith with PMA (Positive Mental Attitude) Faith is state of mind through which your aims, desires, plans and purposes may be translated into their physical or financial equivalent. But Faith without work is dead so BIBLE says.. You should not simply have faith, you must add to your faith hard and consistent work.
Scenario: Meningitis <ul><li>ABC breathing spontaneously rr 18/min 4l O2 via mask, sats 90%; pulse 110 bpm reg small volume; BP 90/60 mmHg T39.6C </li></ul><ul><li>GCS - E2V3M4 </li></ul><ul><li>Detailed check - petechiae non blanching rash trunk, buttocks, Neck stiffness </li></ul><ul><li>Small contusion L temperoparietal area </li></ul><ul><li>Capillary refill time > 3 secs, peripheral cyanosis+ </li></ul><ul><li>Brudzinski sign positive </li></ul><ul><li>Ix skin scraping from lesion : gram negative diplococci ; CSF gram negative diplococci; FBC wcc 18 (polymorhic leucocytosis ) </li></ul> Scenario: Meningitis <ul><li>ABC breathing spontaneously rr 18/min 4l O2 via mask, sats 90%; pulse 110 bpm reg small volume; BP 90/60 mmHg T39.6C </li></ul><ul><li>GCS - E2V3M4 </li></ul><ul><li>Detailed check - petechiae non blanching rash trunk, buttocks, Neck stiffness </li></ul><ul><li>Small contusion L temperoparietal area </li></ul><ul><li>Capillary refill time > 3 secs, peripheral cyanosis+ </li></ul><ul><li>Brudzinski sign positive </li></ul><ul><li>Ix skin scraping from lesion : gram negative diplococci ; CSF gram negative diplococci; FBC wcc 18 (polymorhic leucocytosis ) </li></ul>
Neck Stiffness: * Pathogenesis: Meningeal irritation. Neck Stiffness: * Pathogenesis: Meningeal irritation.
Brudzinski Sign of Meningitis: * Pathogenesis: Meningeal irritation. Brudzinski Sign of Meningitis: * Pathogenesis: Meningeal irritation.
Kernig’s Sign of Meningitis: * Pathogenesis: Meningeal irritation. Kernig’s Sign of Meningitis: * Pathogenesis: Meningeal irritation.
Pathology of Meningitis Dr. Venaktesh M. Shashidhar Associate Professor & Head of Pathology Pathology of Meningitis Dr. Venaktesh M. Shashidhar Associate Professor & Head of Pathology
Case: <ul><li>38 Year Fijian male </li></ul><ul><li>Headache, Photophobia since 2 months. </li></ul><ul><li>Past history of diabetes – irregular treatment. </li></ul><ul><li>3 days back, drowsy, seizure, vomiting. </li></ul><ul><li>On examination: Bil. Papillary edema </li></ul><ul><li>Responded to Mannitol + steroids </li></ul><ul><li>Died 3 rd day in hospital - respiratory arrest.. </li></ul> Case: <ul><li>38 Year Fijian male </li></ul><ul><li>Headache, Photophobia since 2 months. </li></ul><ul><li>Past history of diabetes – irregular treatment. </li></ul><ul><li>3 days back, drowsy, seizure, vomiting. </li></ul><ul><li>On examination: Bil. Papillary edema </li></ul><ul><li>Responded to Mannitol + steroids </li></ul><ul><li>Died 3 rd day in hospital - respiratory arrest.. </li></ul>
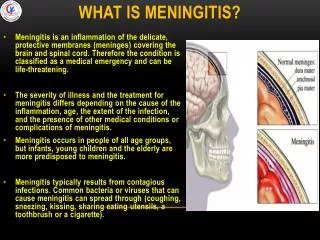
Meningitis: <ul><li>Inflammation of Meninges. </li></ul><ul><li>Leptomeningitis – Subarachnoid & Pia. </li></ul><ul><li>Pachymeningitis – Dura (Local trauma) </li></ul><ul><li>Meningoencephalitis – + Brain. </li></ul><ul><li>Aetiologic Types: </li></ul><ul><ul><li>Infective – Septic & Aseptic (B, V, F & TB) </li></ul></ul><ul><ul><li>Chemical – Drugs. </li></ul></ul><ul><ul><li>Carcinomatous – metastasis. </li></ul></ul> Meningitis: <ul><li>Inflammation of Meninges. </li></ul><ul><li>Leptomeningitis – Subarachnoid & Pia. </li></ul><ul><li>Pachymeningitis – Dura (Local trauma) </li></ul><ul><li>Meningoencephalitis – + Brain. </li></ul><ul><li>Aetiologic Types: </li></ul><ul><ul><li>Infective – Septic & Aseptic (B, V, F & TB) </li></ul></ul><ul><ul><li>Chemical – Drugs. </li></ul></ul><ul><ul><li>Carcinomatous – metastasis. </li></ul></ul>
Septic Meningitis: common causes S. pneumoniae , N. meningitidis , Mycobacteria, Cryptococci Adults N. meningitidis , S. pneumoniae Children Neisseria meningitidis, Haemophilus influenzae, Streptococcus pneumoniae Infants Group B Streptococci, Escherichia coli , Listeria monocytogenes Neonates Causes Age Septic Meningitis: common causes S. pneumoniae , N. meningitidis , Mycobacteria, Cryptococci Adults N. meningitidis , S. pneumoniae Children Neisseria meningitidis, Haemophilus influenzae, Streptococcus pneumoniae Infants Group B Streptococci, Escherichia coli , Listeria monocytogenes Neonates Causes Age
. Pneumococcal Meningitis: Retraction of dura reveals leptomeninges which are edematous and have multiple small hemorrhagic foci (red) note greenish pus covering brain.
. Viral Meningitis: Perivascular cuffs of lymphocytes and Microglial nodules
. HIV Meningoencephalitis: Perivascular Lymphocytes Microglial nodule and multinucleated giant cells
. HIV Encephalitis: Perivascular lymphocytic cuff, Microglial nodule & Giant Cells.
. Herpes Encephalitis: Destruction of inferior frontal and anterior temporal lobes – necrotizing inflammation
. Septic Meningitis - Organisms Organism causing meningitis vary with the age of the patient
. Meningitis: <ul><li>Clinical Features: </li></ul><ul><ul><li>Headache + Neck stiffness. </li></ul></ul><ul><ul><li>Neurological deficits. </li></ul></ul><ul><li>Complications: </li></ul><ul><ul><li>Acute : Encephalitis, Cerebral infarction, Edema, herniation. </li></ul></ul><ul><ul><li>Late: Abscess, subdural empyema, epilepsy. </li></ul></ul><ul><ul><li>Leptomeningeal fibrosis and consequent hydrocephalus </li></ul></ul>
. Brain Abscess: Cerebral abscess. Ring enhancement of developing pseudocapsules, budding of ‘daughter’ lesions, and marked hypodensity of adjacent white matter reflecting severe edema are all characteristic of cerebral abscesses on CT or MR study.
. Brain Abscess: CT Scan Ring enhancement. Surrounding area of inflammation & edema
. Infarction Meningoencephalitis: Mucormycosis in a Diabetic.
. CSF-Examination Norm Septic Viral TB Opalescent (cob-web) Low High > lymph Clear normal High > Lymph Turbid Low High > Poly Clear colorless 2.7-4.0 (n) 0.1-0.4(n) 0-4 lympho Appearance Glucose Protein Cells
. <ul><li>What is a Problem? </li></ul><ul><li>Gap between where you are now and where you want to be. (Hayes 1989) </li></ul><ul><li>How do you solve Problem? </li></ul><ul><li>Mental activity leading from where you are to a more desired ‘goal state’ (Kurfiss 1988) </li></ul>
. Clinical details: <ul><li>38 Year Fijian male </li></ul><ul><li>Headache, Photophobia since 2 months. </li></ul><ul><li>Past history of diabetes – irregular treatment. </li></ul><ul><li>3 days back, drowsy, seizure, vomiting. </li></ul><ul><li>On examination: Bil. Papillary edema </li></ul><ul><li>Responded to Mannitol + steroids </li></ul><ul><li>Died 3 rd day in hospital - respiratory arrest </li></ul><ul><li>Brain sections after limited autopsy. </li></ul>
. Autopsy <ul><li>Marked inflammtory infiltrate in meninges </li></ul><ul><li>Superficial Cerebral edema (cortex) </li></ul>
. Meningitis - Cryptococci <ul><li>Round capsulated fungal organisms </li></ul><ul><li>Lymphocytic infiltrate around </li></ul>
. Cryptococcal Encephalitis: Tiny refractile yeasts
. Cryptococcal Meningitis: Special stains for cryptococci: PAS; Silver stain India Ink: Double refractile spherules with clear halo
. Cryptococcal Meningitis: <ul><li>chronic basal leptomeningitis. </li></ul><ul><li>Opaque thick fibrotic </li></ul><ul><li>CSF obstruction - hydrocephalus. </li></ul><ul><li>Gelatinous material within the subarachnoid space and small cysts within the parenchyma ("soap bubbles") </li></ul><ul><li>Specially in the basal ganglia. </li></ul>
. Summary: <ul><li>Leptomeningitis, Pachymeningitis. </li></ul><ul><li>Head ache, Neck stiff ness. </li></ul><ul><li>Common causes, organisms. </li></ul><ul><li>Septic, Viral & TB – CSF findings. </li></ul><ul><li>Infective, Chemical Carcinomatous </li></ul><ul><li>Complications – Acute / Chronic </li></ul><ul><li>Edema, herniation, infarction, abscess, hydrocephalus. </li></ul>
. Formerly, when religion was strong and science weak, men mistook magic for medicine. Now when science is strong and religion weak, men mistake medicine for magic…!
. CPC-3.7– CNS –Tumors/men. <ul><li>Pathology - Core Learning Issues: </li></ul><ul><ul><li>Pathology of common Primary and secondary CNS tumours in different age groups. </li></ul></ul><ul><ul><li>Over view of epilepsy – include rare causes like neurofibromatosis, sturge weber, tuberous sclerosis - x . </li></ul></ul><ul><ul><li>Genetic basis for idiopathic epilepsy - x </li></ul></ul><ul><ul><li>Increased intracranial pressure – Pathogenesis & pathology. </li></ul></ul><ul><ul><li>Meningitis – Overview, common types & Pathology. </li></ul></ul><ul><li>Basic science - Core Learning Issues: </li></ul><ul><ul><li>Causes ‘break through’ seizures in patients with epilepsy </li></ul></ul><ul><ul><li>Mechanism of action for seizures caused by drug/alcohol withdrawal </li></ul></ul><ul><ul><li>Mechanism of action for seizures caused by drug overdose (cocaine, amphetamine, tricyclic antidepressants) </li></ul></ul><ul><ul><li>Mechanism of action for seizures caused by metabolic disturbance : hypoglycaemia; hypo + hyper natraemia; hypo- and hypercalcaemia; uraemia </li></ul></ul>
. 28y M, Fever, meningitis ? type <ul><li>Viral </li></ul><ul><li>Fungal </li></ul><ul><li>Bacterial </li></ul><ul><li>Carcinomatous </li></ul><ul><li>Pick’s disease </li></ul>
. 28y M, Fever, meningitis ? type <ul><li>Viral </li></ul><ul><li>Fungal </li></ul><ul><li>Bacterial </li></ul><ul><li>Carcinomatous </li></ul><ul><li>Pick’s disease </li></ul>
. 60 Year rapid dementia… <ul><li>A 66-year-old woman vocalist complains of difficulty remembering her favorite songs. This problem continues to worsen over the next several months, and the patient becomes increasingly withdrawn from her family. When examined, she evidences dementia and gait disturbance. MRI demonstrates mild cerebral atrophy. Analysis of CSF shows no inflammatory cells and normal levels of glucose and protein. An EEG reveals periodic spike-wave complexes. One month later, the patient is bedridden and nonresponsive. A brain biopsy is performed and the results are shown. </li></ul>
. 66y Woman rapid dementia… ? diagnosis <ul><li>Primary Amyloidosis. </li></ul><ul><li>Alzheimers disease. </li></ul><ul><li>Creutzfeldt-Jakob disease </li></ul><ul><li>Multi-infarct dementia </li></ul><ul><li>Pick’s disease </li></ul>