Download
1 / 97
1.16k likes | 6.12k Views
Presentation about 'Pathology of Pneumonia'

E N D
Pathology of Pneumonia Pneumonia 9/3/2006 …….. I have no concerns that this group of students are in any way resting on their laurels. So far the feedback from the medical staff has been excellent. There have been a number of preceptors who have noted the substantial difference between this years 4th yrs and last years 4th yrs. A number of their preceptors in the hospital, who are not easily impressed, have gone out of their way to tell me how impressed they have been with this group. ………… Impressive….! Keep it up…..! 1
Pneumonia CPC-4 Mr. Turner is a 38 years old Vietnamese cane farmer living near Cairns. He is married to an indigenous woman and has 2 children aged 10 and 12. He is sent by his GP to A&E with high fever, shortness of breath and cough. He feels very unwell and is flushed and feeling breathless and faint. 2 Pneumonia CPC-4 Mr. Turner is a 38 years old Vietnamese cane farmer living near Cairns. He is married to an indigenous woman and has 2 children aged 10 and 12. He is sent by his GP to A&E with high fever, shortness of breath and cough. He feels very unwell and is flushed and feeling breathless and faint. 2
Pneumonia CPC-4 Questions: Duration, course, sputum, wt loss. Past history, Family Smoking, recent contacts/visits. Diabetes, sexual/venereal diseases. Differential diagnoses: Cardiovascular – MI, CCF, etc.. Respiratory – Pneumonia, Bronchiolitis, aspiration/inhalation injury, Asthma, ARDS, Pulm. Embolism, Empyema. Metabolic – Acidosis, Diabetic, Septicemia – focus of infection? AIDS, Q fever, Legionella. Others: Cystic Fibrosis, Immunodeficiency. 3 Pneumonia CPC-4 Questions: Duration, course, sputum, wt loss. Past history, Family Smoking, recent contacts/visits. Diabetes, sexual/venereal diseases. Differential diagnoses: Cardiovascular – MI, CCF, etc.. Respiratory – Pneumonia, Bronchiolitis, aspiration/inhalation injury, Asthma, ARDS, Pulm. Embolism, Empyema. Metabolic – Acidosis, Diabetic, Septicemia – focus of infection? AIDS, Q fever, Legionella. Others: Cystic Fibrosis, Immunodeficiency. 3
Pneumonia Pathogenesis of Clinical features: Tachypnoea, Dyspnoea, Resp Acidosis Solid/airless lungs – decreased oxygenation. Dull percussion - Consolidation – Exudation Rusty sputum – RBC+WBC (LRT bleed), S.pneum, Greenish sputum – Pseudomonas. Foul smelling sputum- anaerobic. Current jelly sputum-Klebsiella. Fever – Inflammatory mediators. 4 Pneumonia Pathogenesis of Clinical features: Tachypnoea, Dyspnoea, Resp Acidosis Solid/airless lungs – decreased oxygenation. Dull percussion - Consolidation – Exudation Rusty sputum – RBC+WBC (LRT bleed), S.pneum, Greenish sputum – Pseudomonas. Foul smelling sputum- anaerobic. Current jelly sputum-Klebsiella. Fever – Inflammatory mediators. 4
Pneumonia "In the presence of greatness, pettiness disappears. In the absence of a great dream, pettiness prevails." Robert Fritz Composer, Filmmaker and Author 5 Pneumonia "In the presence of greatness, pettiness disappears. In the absence of a great dream, pettiness prevails." Robert Fritz Composer, Filmmaker and Author 5
Pathology of Lung Infections Dr. Venkatesh M. Shashidhar Assoc. Prof & Head of Pathology Pathology of Lung Infections Dr. Venkatesh M. Shashidhar Assoc. Prof & Head of Pathology
Pneumonia Normal Lung Tr.Air Sh Br. Mar. 7 Pneumonia Normal Lung Tr.Air Sh Br. Mar. 7
Normal Lung Type 2 Type 1-Pneumocyte Normal Lung Type 2 Type 1-Pneumocyte
Pneumonia Respiratory system: Introduction 5000 sq meters of area….! (olympic track) Filters >10,000 L of air / day…! Normal lungs are sterile. Delicate, thin resp. mem – gas exch. Filter, humidify, sterilize, highly sensitive. RTI – commonest in medical practice. Pathology: Injury, Infections & Neoplasia. Acute / Chronic. Disorders of Airway – Bronchitis, COPD, Asthma, tumors. Disorders of Lung tissue –Pneumonia, Pneumoconiosis. 9 Pneumonia Respiratory system: Introduction 5000 sq meters of area….! (olympic track) Filters >10,000 L of air / day…! Normal lungs are sterile. Delicate, thin resp. mem – gas exch. Filter, humidify, sterilize, highly sensitive. RTI – commonest in medical practice. Pathology: Injury, Infections & Neoplasia. Acute / Chronic. Disorders of Airway – Bronchitis, COPD, Asthma, tumors. Disorders of Lung tissue –Pneumonia, Pneumoconiosis. 9
. Pneumonia Patterns of Lung disorders: Airway Bronchitis, Bronchiectasis, Bronchiolitis. Tumors / Cancer Parenchyma Pneumonia. * Infections Lung abscess, TB Hyaline membrane dis (HMD & ARDS) Pneumoconiosis Tumors / Cancer Pleura: Pleural effusion (TB) Tumors / Cancer 10
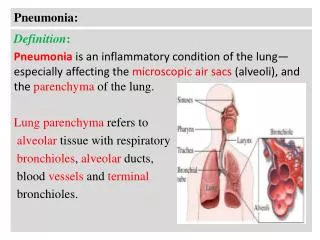
. Pneumonia Pneumonia: Definition & Etiology Inflammation of Lung tissue (not Bronchi) LRT/Distal airways – Alveoli & Terminal bronchioles Decreased defense / Strong Pathogen Immunodeficiency, damaged lung (COPD), Virulent infection - Lobar pneumonia Defective Clearing mechanism Cough/gag Reflex – Coma, paralysis, sick. Mucosal Injury – smoking, toxins, aspiration. Low Alveolar defense - Immunodeficiency Pulmonary edema – Cardiac failure, embol. Obstructions – foreign body, tumors, cystic fibrosis. 11
. Pneumonia Pneumonia Types: Etiologic Types: Morphologic types: Lobar Infective Broncho Viral Interstitial Bacterial Fungal Duration: Acute Tuberculosis Chronic Non Infective Clinical: Toxins Primary / secondary. chemical Typical / Atypical Aspiration Community a / hospital a 12
. Pneumonia Broncho – Pneumonia - Lobar Extremes of age. Middle age – 20-50 Secondary, in sick. Primary in a healthy adult. Both genders. males common. Staph, Strep, H.infl. 95% pneumococcus (Klebs.) Patchy consolidation Entire lobe consolidation Around Small Bronchi Diffuse Not limited by anatomic Limited by anatomic boundaries. boundaries. Usually bilateral. Usually unilateral 13
. Pneumonia Etiologic agents in Pneumonia: 14
. Pneumonia Common Pathogens: Community-Acquired Acute Pneumonia: Strep, H.influenzae, Staph aureus, Klebsiella. Community-Acquired Atypical Pneumonia: Mycoplasma, Chlamydia, SARS* Nosocomial Pneumonia: Klebsiella spp., Serratia, E coli. Aspiration Pneumonia: Anaerobic oral flora (Bacteroides) Chronic Pneumonia: Nocardia, Actinomyces, TB, Atyp. Mycob. Fungal Necrotizing Pneumonia and Lung Abscess: Anaerobic bacteria (foreign body, tumor) Pneumonia in the Immunocompromised: CMV, Pneumocystis, Atyp. Mycob. Fungal. (candida, aspergillus). 15
. Pneumonia Agar? Morphology? diagnosis? Further tests? 16
. Pneumonia Pathogenesis of infective Pneumonia: Step 1: Entry Aspiration Inhalation Inoculation Colonization Hematogenous Direct spread 17
. Grey Hepatization Resolution Pathogenesis of Pneumonia Congestion Red Hepatisation
. Pneumonia Lobar Pneumonia: whole lobe, exudation - consolidation 95% - Strep pneum.(Klebsiella in aged, DM, alcoholics) High fever, rusty sputum, Pleuritic chest pain. Four stages: (*also in bronchopneumonia) Congestion – 1d – vasodilatation congestion. Red Hepatization 2d Exudation+RBC Gray Hepatizaiton 4d neutro & Macrophages. Resolution – 8d few macrophages, normal. 19
. Pneumonia Lobar Pneumonia: 20
. Pneumonia Lobar Pneumonia: Red Hepatization 21
. Pneumonia Lobar Pneumonia: Grey Hepatization 22
. Pneumonia Lobar Pneumonia: Grey Hepatization 23
. Pneumonia Lobar Pneumonia: 24
. Pneumonia Left lower Lobar Pneumonia: 25
. Pneumonia Lobar Pneumonia: 26
. Pneumonia Left lower Lobar Pneumonia: Methylene blue stain: 27
. Pneumonia Lobar Pneumonia – Gray hep… 28
. Pneumonia Lobar Pneumonia – Acute Fibrinous pleurisy 29
. Pneumonia Lobar Pneumonia: 30
. Pneumonia Lobar Pneumonia: Microscopy: Congestion red hepatization 31
. Pneumonia Lobar Pneumonia: Red hepatization. • Acute inflammatory cells & RBC Filling alveolar spaces Uniformly. • Congested capillaries in the alveolar septa 32
. Pneumonia Lobar Pneumonia: Red hepatization. • Acute inflammatory cells. Filling alveolar spaces Uniformly. • Congested capillaries in the alveolar septa 33
. Pneumonia Lobar Pneumonia: Red Grey hepatization. 34
. Pneumonia Lobar Pneumonia: Grey hepat. 35
. Pneumonia Lobar Pneumonia: 36
. Pneumonia Lobar Pneumonia: 37
. Pneumonia Lobar Pneumonia: Which lobe? 38
. Pneumonia Broncho- pneumonia 39
. Pneumonia Broncho- pneumonia 40
. Pneumonia Broncho- pneumonia 41
. Pneumonia Bronchopneumonia (patchy) Extremes of age. (infancy and old age) Secondary to Risk factors. Staph, Strep, Pneumo & H. influenza Patchy consolidation – not limited to lobes. Suppurative inflammation Usually bilateral More in Lower lobes 42
. Pneumonia Broncho Pneumonia 43
. Pneumonia Bronchopneumonia: 44
. Pneumonia Bronchopneumonia - CT 45
. Pneumonia Bronchopneumonia 46
. Pneumonia Interstitial / atypical Pneumonia Primary atypical pneumonia in the immunocompetant host (Mycoplasma or Chlamydia) Interstitial pneumonitis immunocompromised host : Pneumocystic carinii; CMV Immunocompetant host: Influenza A Gross features: Lungs are heavy but not firmly consolidated Microscopic features: Septal mononuclear infiltrate Alveolar air spaces either ‘empty’ or filled with proteinaceous fluid with few or no inflammatory cells 48
. Pneumonia Interstitial Pneumonia: Lymphocyte Infiltrate in alveloar wall 49
. Pneumonia Acute viral Pneumonia: Fibrin Lymphocytes B.V 50