Download
1 / 68
680 likes | 690 Views
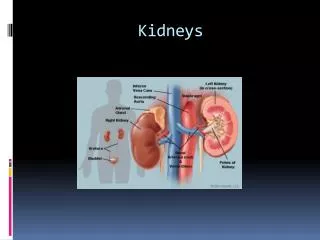
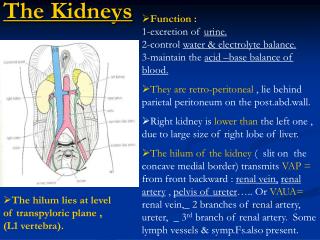
The Kidneys. Function : 1-excretion of urine. 2-control water & electrolyte balance. 3-maintain the acid –base balance of blood. They are retro-peritoneal , lie behind parietal peritoneum on the post.abd.wall.

E N D
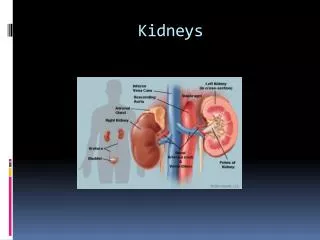
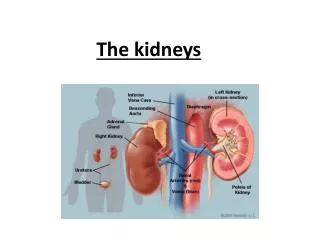
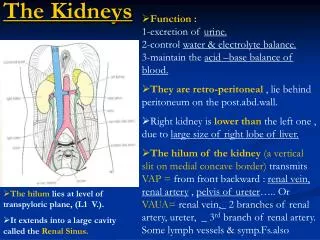
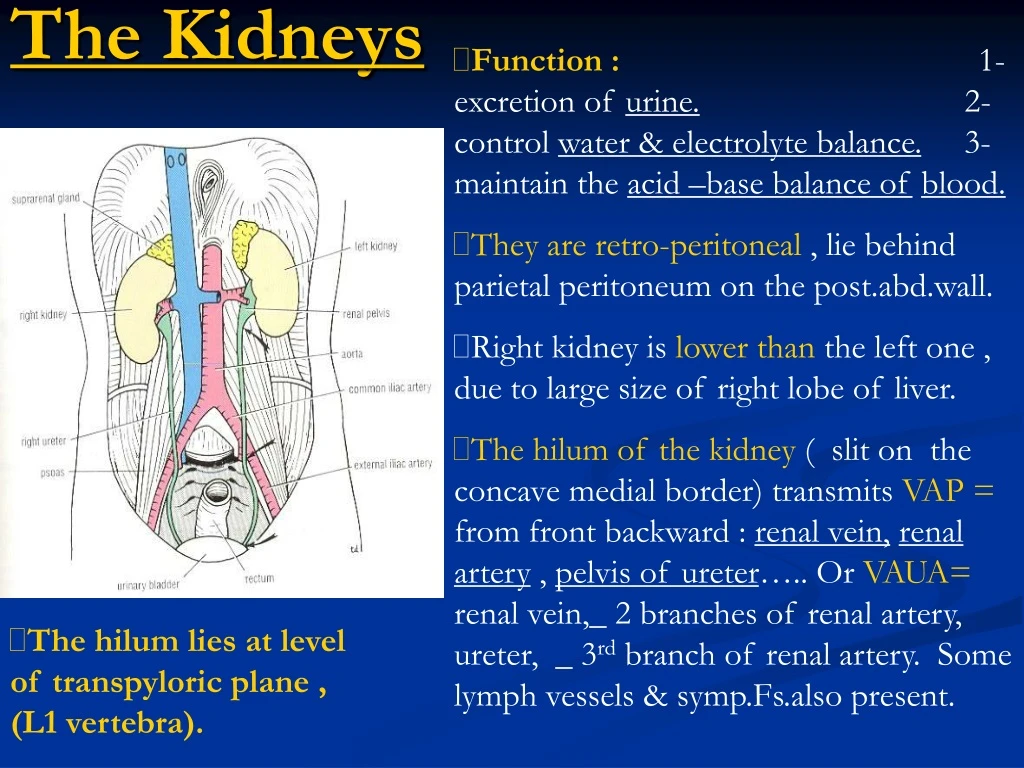
The Kidneys • Function : 1-excretion of urine. 2-control water & electrolyte balance. 3-maintain the acid –base balance ofblood. • They are retro-peritoneal , lie behind parietal peritoneum on the post.abd.wall. • Right kidney is lower than the left one , due to large size of right lobe of liver. • The hilum of the kidney ( slit on the concave medial border) transmits VAP = from front backward : renal vein,renal artery , pelvis of ureter….. Or VAUA= renal vein,_ 2 branches of renal artery, ureter, _ 3rd branch of renal artery. Some lymph vessels & symp.Fs.also present. • The hilum lies at level of transpyloric plane , (L1 vertebra).
The Kidneys : • The kidneys extend from T12V toL3 vertebra. They recive some protection from lower part of rib cage. • Left kidney is slightly higher than right one , it reaches 11th rib ,while the right kidney reaches only 11th intercostal space (due to presence of liver).
Coverings of the Kidney : • Fibrous capsule : it is closely attached to its outer surface. • Peri-renal fat : it covers the fibrous capsule. • Renal fascia : it is a condensation of C.T. surrounding the peri-renal fat and encloses the kidneys & suprarenal glands. • Para-renal fat : lies external to renal fascia. • Peri-renal fat , renal fascia ,andpara-renal fat support the kidneys and held them in position on post.abd.wal.
Each kidney has a light brown outer cortex , and a dark brown inner medulla. • The medulla is composed of about a dozenrenal pyramids, with base toward the cortex and apex ( renalpapilla) projecting medially. • The pyramids are separated by extensions of cortex called renal columns. Extending Fs.from the bases of renal pyramids into cortex are striations called medullary rays. • Renal pelvis or (pelvis of ureter) is a funnel-shaped dilatation, which is formed in the sinus of kidney by union of 2-3 majorcalyces, Each major calyx divides into 2 or 3 minor calyces. It passes through hilum. • Each minor calyx is indented by tha apex of the renal pyramid ,(renal papilla). Renal Structure : A.ant.surface of Rt.kidney. B. coronal section showing cortex, medulla, pyramids, renal papillae and calyces. C .showing the Nephrons & blood vessels within the kidney.
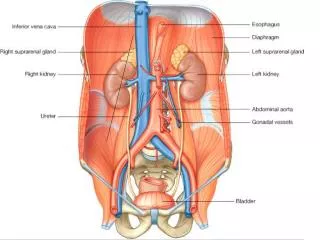
Anterior relation of the Kidneys : Right Kidney : • Suprarenal gland , liver , second part of duodenum , right colic flexure, coils of jejunum. Left Kidney : • Suprarenal gland , spleen , stomach, pancreas , left colic flexure & descending colon , coils of jejunum.
Peritoneal Covering of the Kidney : • The anterior surface only of right kidney is covered with peritoneum except : 1- supra-renal area. 2- duodenal area. 3- colic area. • The anterior surface only of left kidney is covered with peritoneum except : 1- supra-renal area. 2- pancreatic area. 3- area of descending colon.
Posterior Relations of the kidneys : Right Kidney : • Diaphragm ,, 12th rib , psoas ,quadratus lumborum & transversus abdominis ms. Subcostal (T12), iliohypogastric, & ilioinguinal nerves (L1), run downward and laterally. Left Kidney : • Diaphragm, 11th & 12th ribs. The other structures as the right kidney.
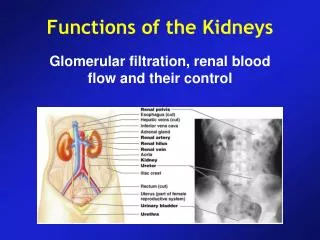
Blood Supply of the Kidney : • At level of L2 V.-renal artery arises from aorta. Each renal artery divides into 5 segmental arteries 4- in front & 1- behind the renal pelvis. • Lobar arteries arise from each segmental artery, one for each renal pyramid. • 2 or 3 -Interlobar arteries arise from each lobar artery , running on each side of renal pyramid. • At the junction of cortex & medulla, interlobar arteries give off arcuate arteries arching over the bases of pyramids, atjunction of cortex & medulla. • Several interlobular arteries arise from arcuate arteries that ascend in the cortex. • Afferent glomerular arterioles arise as branches of interlobular arteries.
Blood supply of Kidneys : • Afferent glomerular arterioles break into capillaries that collect into efferent glomerular arterioles. • Efferent G.arterioles breaks intointerlobular veins ending in arcuate veinsthat collect to interlobar,lobar,renal vein. Eff.G.arterioles also pass deeply into medulla and breaks into vasarecta which pass to apex of pyramid and breaks into capillaries which constitute the venous side and end in arcuate veins, at junction of cortex& medulla. • Arcuate veins collect into inter-lobar veins which collect into lobar then renal vein and finally I.V.C. C-section of kidney, showing position of nephrons & arrangement of Bl.vs. in kidney
Venous , lymphatic drainage & N.Supply : • Veins :Renal vein emerges from hilum in front of renal artery and drains into I.V.C. • Lymph drainage :lateral aorticL.Ns. around origin of renal artery. • N.Supply : -Sympathetic ¶sympathetic via renal plexus surrounding renal artery. –afferent sympathetic Fs.in the renal plexus enter spinal cord segments at T10,11, 12
Ureter (Abdominal part) : • It is a muscular tube that extends from hilum of kidney to post.surfaceof urinary bladder. • It propels urine by peristaltic contractions. • It has 3 constrictions :where renal pelvis joins ureter, where it is kinked as it crosses pelvic brim (bifurcation of common iliac artery), where it pierces bladder wall. • Renal pelvisis funnel-shaped upperpart of ureter, lies in the hilum of kidney and receives major calyces.
Ureter : Course of ureter : • It emerges from hilum of kidney to run vertically downward behind parietal peritoneum,on the psoasmajor ms., which separates it from lumbar transverse processes. • It enters pelvis by crossing bifurcation of common iliac arteryin front of sacroiliac joint, till it reaches level of ischial spine. • It ends in U.B. by openning at supero-lateral angle of trigone.
Anterior relations of RightUreter : • Duodenum & terminal part of ileum. • Superior mesenteric artery & mesentry of small intestine. • Right gonadal vessels. • Right colic & Iliocolic vessels
Posterior relations of Right Ureter : • Right psoas major which separates it from lumbar transverse processes. • Right psoas minor. • Genito-femoral N. • Bifurcation of right common iliac artery.
Anterior relations of Left Ureter : • Sigmoid colon & mesocolon. • Sigmoid vessels. • Left gonadal vessels. • Left colic vessels.
Posterior relations of Left Ureter (as the Right ureter) : • Left psoas major which separates it from lumbar transverse processes. • Psoas minor. • genito-femoral N. • Bifurcation of left common iliac artery.
Blood Supply ,Lymph drainage & N. Supply : • Upper part :renal artery (L2 V.). • Middle part :gonadal artery (testicular or ovarian). • Pelvic part :superior vesicalartery. • Lymph drains to lateral aortic & iliac L.Ns. • N.supply : -Sympathetic & parasympathetic Via Renal ,gonadal & hypogastric plexuses (in the pelvis). -Afferent sympathetic Fs.enter spinal cord segments at T11,12 & L1,2.
2 yellowishretro-peritoneal glands that lie on upper poles of kidneys. • They are surrounded by renalfasciabut separated from kidneys by perirenal fat. • Yellow cortex secrets mineral corticoids & glucocorticoids & sex hormones. • Medulla secrets catecholamines : epinephrine & norepinephrine. • Rt,gland : caps upper pole of Rt.kidney, lies behind Rt.lobe of liver, I.V.C., anterior to diaphragm. • Left gland : reaches hilum of kidney, lies behind pancreas, lesser sac & stomach, anterior to diaphragm. Suprarenal glands
Blood Supply, Lymph & N. Supply of Suprarenal glands : • Arterial supply : inferior phrenic artery (upper part), aorta (middle part) & renal artery (lower part). • Vein of right gland ends in I.V.C., while vein of left gland ends in left renal vein. • Lymph drains into lateral aortic nodes. • N.Supply : symp. Fibres from splanchnic nerves & parasympathetic Fs.
Clinical Notes : 1- Renal pain • Type of pain : dull ache to severe pain in the flank that may radiate into lower abdomen. • Causes : 1-stretching of kidney capsule. 2-spasm of smooth muscle in renal pelvis. • Pain is referred along distribution of subbcostal N.(T12) …. to the flank & anterior abd. Wall., because afferent N.Fs.ascends from renal plexus to spinal cord at level of T12, via lowest splanchnic N.in thorax & symp.trunk.
2- Renal colic : • In renal colic, strong peristaltic waves of contraction pass through ureter in attempt to pass the stone onward, so the spasm of smooth muscle causes an agonising colicy pain. • Renal pelvis & ureter send their afferent nerves into spinal cord segments : T11,12 and L1,2 • Colicy pain is referred to areas supplied by these seg.of spinal cord, into flank, loin & groin. • When stone enters low part of ureter, pain is referred to testis or tip of penis or labium majus in female. • Sometimes ureteric pain is referred to front of thigh along femoral branch of genitofemoral N.(L1,2). • Pain is often so severe that spreads in C.N.S. giving nausea.
3-Ureteric Stone • Ureteric stones are arrested in the ureteric narrowingat these sites :1-at pelvi-ureteral junction. 2-at pelvic brim. 3-at its enterance to urinary bladder. • Most of ureteric stones are not seen by plain radiographic examination, so I.V.pyelography is usually necessary by using of radiopaque compound (iodine-containing compound), by injection into subcut.arm vein, so the coarse of ureter is clearly seen in front oftips of transverse processes of lumbarvertebrae, crossing sacro-iliac joint then ends in bladder.
Abdominal Aorta : • It is a continuation of descending thoracic aorta ,it enters abdomen through aortic opening of diaphragm at the level of T12 vertebra. • It descends behind peritoneum on the bodies of lumbar vertebrae. • it terminates at the level of L4 vertebra (inter-cristal plane) , into 2 common iliac arteries. • On the right side : I.V.C., azygos vein ,lymph trunk (cisterna chyli) + Rt.crus of diaphragm. • On the left side : sympathetic trunk + left crus of diaphragm.
Branches of Abdominal Aorta : • 3 anterior visceral branches : celiac, superior mesentric & inferior mesenteric arteries. • 3 lateral visceral branches : suprarenal, renal & gonadal arteries. • 5lateral abdominal wall branches : inferior phrenic & 4 lumbar arteries. • 3terminal branches : 2 common iliac + median sacral artery.
Single Branches of Abdominal Aorta : • Coeliac artery : from front of aorta at the level of T12 V. (or upper border of L1 V) • Superior mesentric artery : from front of aorta at the level of L1 V.(transpyloric plane). • Inferior mesenteric artery : from front of abdominal aorta at level of L3 V. (subcostal plane). • Median sacral artery : from back of abdominal aorta at the level of L4 V.
Paired Branches of Abdominal Aorta : • Phrenic arteries :at the sides ofcoeliac artery (at level of upper border of L1 V.,or T12V.) • Middle suprarenal arteries(at lower border of L1 V.) • Renal arteries (at L2) • Testicular or ovarian arteries : on the sides of inferior mesenteric artery (at level of L3V). • Lumbar arteries : 4 pairs of arteries, arising from back of aorta. • Common iliac arteries : at level of L4 V. (inter-cristal plane)
Terminal Branches of Abdominal Aorta : • Common iliac arteries : they ariseat level of L4 V ,descend downward and laterally along medial border of Psoas major. • Each common iliac artery crossed anteriorly by the ureter & ends in front of sacro-iliac joint into external &internal branches.
Branches of Common iliac artery: 1-External iliac artery : -runs along medial border of Psoas major. • It enters thigh behind inguinal ligament to become femoral artery. • It gives off 2 branches above inguinal ligament :1-inferior epigastric artery. 2-deep circumflex iliac artery. • Inferior epigastric artery passes medially along medial margin of deep inguinal ring and enters rectus sheath behind rectus abdominis to anastomose with superior epigastric artery to supply anterior abd.wall. • Deep circumflex iliac artery ascends laterally to iliac crest to supply Ms. of anterior Abd.wall 2-Internal iliac arterydescends topelvis in front of sacro-iliac joint.
Obliteration of abdominal aorta & iliac arteries : • Atherosclerosis leads to gradual occlusion of bifurcation of abdominal aorta & iliac arteries, results in pain inleg during walking(claudication) due to lack of blood in external iliac artery & impotance due to lack of blood in internal iliac arteries. • Some collateral circulation is established, but it is physiologicallyinadequate, so skin ulcer & tisssue death may occur. • Surgical treatment by thrombo-end-arterectomy or a bypass graft should be done.
Obliteration of abdominal aorta & iliac arteries : • Note the possible collateral circulation of abdominal aorta. • Note great dilatation of mesentericarteries& their branches, which occurs if the aorta is slowly blocked just below level ofrenal arteries (L2).
Course of I.V.C. : • It is formed by union of the 2 common iliacveins behind right common iliac artery at level of L5 vertebra (intertubercular plane), 1 inchto right of median plane. • It ascends on right side of aorta to pierce central tendon ofdiaphragmat level of T8vertebra to drain into right atrium ofheart.
Tributaries of I.V.C : • 2 anterior visceral tributaries : the 2 hepatic veins. • 3 lateral visceral tributaries : -Rt.suprarenal V. (left drains into left renal vein). -renal veins. -Rt.gonadal V. (left drains into left renal vein). • 5 lateral abdominal wall tributaries : -inferior phrenic veins. -4 lumbar veins. • 3 veins of origin :2 commoniliac veins + median sacral vein.
Medial & lateral Relations of I.V.C. : • Medially( on left side) : abdominal aorta. • Laterally (on right side) : right ureter.
Anterior relations of I.V.C. : • Right common iliac artery. • Root of mesentry & superior mesenteric vessels. • 3rd part of duodenum. • Right testicular or ovarian Ar. • Head of pancreas. • 1st part of duodenum. • foramen to lesser sac separates I.V.C. from _ portal vein, hepatic artery & bile duct in free right margin of lesser omentum.
Foramen to lesser sac : • Note that opening to lesser sac (epiploic foramen at level of transpyloric plane L1) separates I.V.C. from portal vein. • Venous blood from abdominal part of G.I.T.drains to liver by portal vein,then from hepatic veins to I.V.C.
Posterior relations of I.V.C. : • Bodies of lumbar vertebrae. • Right sympathetic trunk. • Right psoas major. • Right lumbar arteries. • Right renal, suprarenal & phrenic arteries. • Right crus of diaphragm.
Inferior Mesenteric Vein : • It begins halfway down anal canal as a continuation of superior rectal vein. • It is a tributary of portal circulation. • It joins splenic vein behind body of pancreas. • It receives tributaries related to branches to the artery (left colic, sigmoid, & sup.rectal veins)
Splenic Vein : • It is a tributary of portal vein. • It begins at hilum of spleen by union of several splenic veins and is joined byshort gastric & left gastro-epiploic veins. • It passes within splenicorenal ligament with splenic artery ( the artery lies along upper border of pancreas) ,then runs behind body of pancreas to join superior mesentric Vbehind neck of pancreas to form portal vein. • It is joined bypancreatic veins & inferior mesenteric vein.
Superior Mesenteric Vein : • It is a tributary of portal vein. • It begins at ileocecal junction lying within root of mesentry ofsmall intestine on right side of the artery. • It passes in front of 3rd part of duodenum , behind neck of pancreas, where it joins splenic vein to form portal vein. • It receives tributaries correspond to the artery (middle colic, right colic, iliocolic & jejunal and ileal veins).
Note tributaries of the Portal vein. • Portal vein drains blood from abdominal part of G.I.T. from lower 1/3 ofesophagusto halfway down the anal canal, it also drains blood from spleen,pancreas, & gallbladder. • Portal vein enters liver and breaks into sinusoids, from which blood passes into hepatic veins that drain into I.V.C.
External iliac vein : • It begins behind inguinal ligament as a continuation of femoral vein. • It ends by joining internal iliac vein to form common iliac vein. • It receives inferior epigastric & deep circumflex iliac veins.
Internal iliac vein : • It begins in the pelvis by joining all tributaries that correspond to branches of the artery. • It ends in front of sacroiliac joint by joining external iliac vein to form common iliac vein. • The 2 common iliac veins joined together to form I.V.C. (at L5V.)
Collateral venous anastomoses between I.V.C. & S.V.C. : • Temporary varicose veins , result from compression of I.V.C. by enlarged uterus during later stages of pregnancy. • Malignant retro-peritoneal tumors causeblockage of I.V.C., resulting in dilatation ofextensive anastomoses of the tributaries of I.V.C. (as lumbar, Azygos & hemiazygos veins). • This alternative pathway for blood to return to right atrium is commonly referred to as caval-caval shunt. • The same pathway results in case of Sup.mediastinal tumor, compressing S.V.C Clinically : enlarged subcutaneous anastomosis is seen on thoracabdominal wall between lateral thoracic vein (tributary of axillaryvein) & superficial epigastric vein. (tributary of femoral vein).
Collateral venous anastomoses between I.V.C. & S.V.C. : • Note the alternative pathways for blood to return to right atrium if S.V.C. becomes blocked below enterance of Azygos vein, through azygos, internal or lateral thoracic veins into I.V.C. • Similar pathways exist if I.V.C.becomes blocked below renal veins. • So,a number of anastomotic channels connect both venae cavae indirectly in case of thrombosis of any vein • Note also anastomosis betweenportal & systemic veins in anal canal.
Sympathetic trunk (Abdominal part) : • It is continuous above with thoracic part & below with pelvic part of symp.trunk. • It enters abdomen behind medial arcuate ligament. • It descends along medial border of psoasmajor, lying on the bodies of lumbarvertebrae. • it enters pelvis behind common iliac vessels. • Right symp.trunk lies behindI.V.C., but left symp.trunk lies close to left border of aorta. • It has 4 or 5 ganglia, 1st & 2nd often being fused together. Aorta and related sympathetic plexuses.