Download
1 / 38
380 likes | 446 Views
Transient Cardiac Disease Rachel Aubrey. Medications: Insulin Inhibace plus Metoprolol Aspirin Calcium Alu-tabs Neorecormon NKDA. Patient One . 54yo man presents with chest pain. PmHx: T2DM CKD – stage IV- V kidney disease, eGFR 15%, due to start peritoneal dialysis HTN Ex smoker

E N D
Transient Cardiac Disease Rachel Aubrey
Medications: Insulin Inhibace plus Metoprolol Aspirin Calcium Alu-tabs Neorecormon NKDA Patient One .54yo man presents with chest pain • PmHx: • T2DM • CKD – stage IV- V kidney disease, eGFR 15%, due to start peritoneal dialysis • HTN • Ex smoker • High BMI
Patient One .54yo man presents with chest pain • HxPC: • Pain is sharp located in the anterior and central chest radiating to the neck and shoulders. Onset 4 hours ago, took paracetamol at home with nil effect. Ongoing so presents to ED. • Associated with dyspnoea, no nausea or diaphoresis. • Worse when laying flat, with inspiration and swallowing. • Chronic peripheral oedema unchanged. • No calf pain or swelling, prolonged immobility/surgery, haemoptysis, history of malignancy, history of VTE. • Possible fevers at home. • No cough/cold/ coryza or gastrointestinal symptoms. • Longstanding history of poor exertional capacity with occasional chest pain, normal ETT 3 years ago.
HS dual + added sounds JVP 4-5cm Peripheral oedema and pitting to knees Chest: reduced AE bases and few creps Abdomen SNT Patient One .54yo man presents with chest pain • O/E: • HR: 114bpm • RR: 24bpm • SpO2: 96% o/a • BP: 145/82 (L) 147/88 (R) • Temp: 37.4
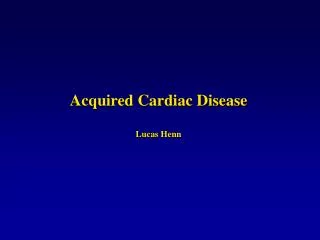
Patient One .54yo man presents with chest pain Widespread concave ST elevation and PR depression is present throughout the precordial (V2-6) and limb leads (I, II, aVL, aVF). There is reciprocal ST depression and PR elevation in aVR
U&E: Cr 500 Urea 32 Na 131 K 5.9 Troponin T 62, (prev 45) CRP 82 Patient One .54yo man presents with chest pain • Bloods: • FBC: • Hb 106 • WCC: 13.4 • Neut: 8.6 • Plt: 268
PA: No significant pulmonary venous congestion, Increased CTR, “globular” or “flask shaped” Lateral: Loss of retrosternal clear space, “Fat-pad” sign - “Oreo” sign, Pleural effusion
Acute inflammation of pericardium Exudate in pericardial space, usually contains only 15-50mls Inflammatory cells -mainly PMN – leukocytes Fibrinous with adhesion formation Can be serous or haemorrhagic ~ 5- 8% of ED presentations with CP without MI M > F , adults > children ~80% are post-viral or idiopathic Pericarditis
Medications: Hydralazine* Methyldopa Procainamide* Minoxidil Other: Idiopathic (procedures) Blunt or penetrating Post-MI (Dressler’s syndrome)* Myocardial infarction Uraemia * * Common causes Causes • Infectious: • Viral (HIV, CMV, coxsackie*) • Bacterial (tuberculosis) • Fungal Inflammatory: • SLE* • Scleroderma • ANCA-associated vasculitis Metabolic: • Hypothyroidism Neoplastic: • Metastatic • Primary
Manifestations of pericarditis before RRT or within 8 weeks of starting (dialysis pericarditis affects those on RRT for > 8 weeks) Common at autopsy 50% or uraemic patients have pericarditis. More common in younger patients and in women. Higher incidence of haemorrhagic effusion Caused by accumulation of uraemic toxins. Good response from dialysis – 76% recover. [ Dialysis – Due to inadequate dialysis, possibly substrates of dialysis, poorer response to dialysis and more likely to be subacute, more likely to be complicated by adhesions] Uraemic Pericarditis
Investigations: Leukocytosis, Elevated ESR/CRP, trop in ~30% ECG: PR segment depression. Widespread concave (‘saddle-shaped’) ST elevation. Reciprocal ST depression and PR elevation in aVR and V1 Absence of reciprocal ST depression elsewhere CXR: Cardiomegaly, pleural effusions 50% Clinical Presentation • Symptoms: • Chest pain – most common, 40-100% (sharp, dull, burning, pressing, radiation -> trapezius ridge, worse on inspiration, lying flat and movement) • Cough, Dyspnoea • Malaise, fevers, • Assymptomatic in 8-30% Physical Signs: • Pericardial Rub 35-85% • Tachypnoea • Tachycardia
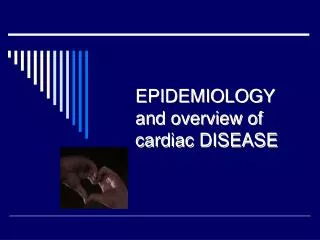
Pericarditis: Generalised ST elevation Presence of PR depression Normal T wave amplitude ST segment / T wave ratio > 0.25 Absence of “fish hook” appearance in V4 ECG changes evolve slowly over time Pericarditis vs Benign Early Repolarization: • Benign Early Repolarization: • ST elevation limited to the precordial Leads • Absence of PR depression • Prominent T waves • ST segment / T wave ratio < 0.25 • Characteristic “fish-hook” appearance in V4 • ECG changes usually stable over time (i.e non-progressive)
Pericarditis Benign Early Repolarization
4 Stages of ECG Changes • Stage 1, seen in the first hours to days. • Diffuse ST elevation (typically concave up) with reciprocal ST depression in leads aVR and V1. There is also an atrial current of injury, reflected by elevation of the PR segment in lead aVR and depression of the PR segment in other limb leads and in the left chest leads, primarily V5 and V6. • Stage 2, typically seen in the first week. • Normalization of the ST and PR segments. • Stage 3, • Development of diffuse T wave inversions, generally after the ST segments have become isoelectric. However, this stage is not seen in some patients. • Stage 4. • Normalization of the ECG or indefinite persistence of T wave inversions ("chronic" pericarditis).
Acute pericarditis is diagnosed by the presence of at least two of the following criteria: Typical chest pain (sharp and pleuritic, improved by sitting up and leaning forward) Pericardial friction rub (a superficial scratchy or squeaking sound best heard with the diaphragm of the stethoscope over the left sternal border) – may need repeat exams. Suggestive changes on the electrocardiogram (typically widespread ST segment elevation) New or worsening pericardial effusion Investigations: bloods inc CRP, ESR, Trop and cultures if febrile, ECG – all CXR – all Echo – tamponade, purrulent infection, myocarditis Diagnosis
Rule out differential causes Stable → Outpatient mx: NSAIDs +/- colchicine If persistent >1 week need further investigation R/V meds – anti coagulants, contributing meds Admit if: Effusion – large, tamponade Fever, leukocytosis, immunocompromised On warfarin Traumatic Trop rise – (myopericarditis) > 1 week, not responding to NSAIDs Management: • Management of complications: • If tamponade is suspected → Echo (gold std) • Tachycardia, tachypnoea, hypotension, signs of hypo-perfusion, distended neck veins, muffled heart sounds, pulsus paradoxus, 'Becks triad' • Pericardiocentesis – sub-xiphoid if emergent. • Restrictive pericarditis requires resection. • Persistent (>1 week) requires further investigation.
HxPC: 60yr old woman was upstairs with her husband who is a patient on a medical ward. During a family meeting she began to report central chest pain and presents to ED immediately. She looks unwell and is taken into monitored. On arrival she reports: - Ongoing retrosternal chest heaviness - Non radiating - Associated nausea and dyspnoea, nil other associated symptoms - Has been otherwise well. PmHx: Hypothyroidism on thyroxine, hyperlipidaemia, No cardiac hx, HTN, T2DM, non smoker and no family hx of IHD - Patient Two 60 year old woman presents with chest pain
Management: Moved to Resus and activate STEMI protocol Quick bedside examination: BP 140/90, HR 80, SpO2 98%, HS dual non added, chest clear IVL placed on the ward and bloods return with troponin T of 140, . Given aspirin, heparin bolus and ticagrelor Transferred to Cath Lab Patient Two 60 year old woman presents with chest pain
Patient Two 60 year old woman presents with chest pain • Troponin T – 140 → 480 • Angiogram: no significant flow limiting lesion, mild coronary artery disease. • Left ventriculography was performed which showed: akinesis of the apical half of the left ventricle and apical ballooning. LVEF was reduced at 35%
Apical Ballooning or Takotsubo Cardiomyopathy • Transient systolic dysfunction of the apical and/or mid segments of the left ventricle that mimics myocardial infarction, but in the absence of obstructive coronary artery disease • Contractile function of the mid and apical segments of the LV are depressed, and there is hyperkinesis of the basal walls, producing a balloon-like appearance of the distal ventricle with systole. • Frequently but not always triggered by an acute medical illness or by intense emotional or physical stress • Pathogenesis unknown. ? catecholamine excess, coronary artery spasm (though few have spasm with Ach provocation), microvascular dysfunction or dynamic mid-cavity or LV outflow tract obstruction. • Mainly post-menopausal women, F >> M, Mean age 61 – 76yrs • ~1-2% of troponin +ve ACS
Clinical Features • Presentation – same as AMI • CP, dyspnoea, ECG changes – often ST elevation and usually in anterior pre-cordial leads 35-55%. Other changes include: deep T wave inversion, QT prolongation, abnormal Q waves, non-specific abnormalities or normal. (Can't distinguish AMI) • Also syncope, arrhythmia, CHF, cardiogenic shock. • Acute HF is more likely in >70yrs, LVEF <40%, presence of physical stressor. • Troponin elevated in 75-85%, usually out of proportion to haemodynamic compromise. • Usually affect LV only. • Diagnosis made on Echo or ventriculography or cardiac MRI – typical appearance. Absence of CAD on angiogram
Management: • Treat as ACS in ED • Primary PCI or fibrinolytic therapy • LV impairement treated as normal – ACEi, B-blockers. • If shock present → USS to look for LVOT obstruction • If present (~15%): NO inotropes, B-blockers, fluid resus • If absent: Cautious use of inotropes -dobutamine & DA • Most recover well over a period of weeks (with regain of normal systolic function), increased risk of recurrance (figure unknown) and long term adreno-receptor blockade may reduce risk of this.
Patient Three26yo woman presents with chest pain and febrile illness • HxPC: • Unwell 8 days with fevers, cough, coryza, myalgias and fatigue. Others at home are unwell with the same – daughter currently admitted with bronchiolitis. • Onset of chest pain 2/7 ago. The pain is anterior, central, sometimes radiating to shoulders and worse with cough and deep inspiration. • Cough with green phlegm. • No palpitations. • SOB has noticed a reduced exertional capacity. • Has been sleeping on 3 pillows for the past 2 days. • No leg swelling. • Amoxycillin by GP 4/7 ago, not improving. • Previously fit and well
Looks unwell, HS S1, S2 + S3 Dry mucous membranes, JVP 4cm. Calves SNT, no pitting Chest: bilateral exp wheeze, few scattered creps Abdomen: SNT Patient Three26yo woman presents with chest pain and febrile illness • O/E: • HR: 125bpm • BP: 100/60 • RR: 25 • Temp: 38.7 • SpO2: 96% oa
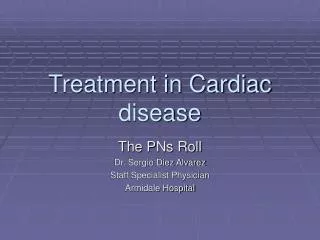
Patient Three26yo woman presents with chest pain and febrile illness
U&E: Na 132 K 3.4 Cr 80 LFTs: ALT 180 AST 166 Otherwise normal *daughter's NPA - adenovirus Patient Three26yo woman presents with chest pain and febrile illness • Bloods: • FBC: • Hb 120 • WCC 18.6 • Neut 11.2 • Plt 540 • Troponin 230 • CRP 113
Myocarditis • Inflammatory infiltrate of the myocardium with necrosis and/or degeneration of adjacent myocytes not typical of the ischemic damage associated with coronary heart disease. • Incidence is unknown. One study suggested that myocarditis is the cause of sudden cardiac death in 8.6% of cases and is identified in up to 9% of routine post-mortem examinations • Multiple causes (see next slide) • Can be acute or chronic • Focal or diffuse (viral usually diffuse, more likely to cause CHF) • Spectrum of disease – assymptomatic → fulminant heart failure (Children more likely to have fulminant, and men more likely to have severe viral myocarditis, fulminant = better prognosis)
Causes • Infectious • Viral infection – most common cause, Coxsackie, adenovirus, parvovirus B19, enterovirus. [less common EBV, Hep, CMV] • Diptheria, fungal, parasitic and rickettsial • Immune mediated • Giant cell, SLE, sarcoidosis, IBD, Kawasaki, + many more • Drug – hypersenstitivity • Clozapine, isoniazid, phenytoin, thiazides + many more • Toxic causes • Drugs: ethanol, cocaine, lithium, • Heavy metal poisoning: lead, copper, iron. • Others: arsenic, insect stings and bites, CO • Physical • Electrical injury, radiation
Findings: fever tachycardia S3 and S4 pericardial rub signs of biventricular failure cardiogenic shock Elevated WCC, CRP, ESR, LFTs ECG: ST, ST elevation, Tw changes – inversion CXR: normal, cardiomegaly or pulm oedema Clinical Features • Presentation: • chest pain • fatigue • SOB • palpitations • fever • malaise • Arthralgias • Arrhyrthmia or sudden death
Requires high level of suspicion as variable presentation. Elevated troponin ECG suggesting myocardial injury or pericarditis Arrhythmia New or unexplained altered cardiac function Particularly in younger patients 20-50yrs +/- viral/infective history – many do not have Initial testing: ECG Troponin/CK Routine labs – though non-specific BNP if uncertain whether CHF present. Diagnosis
Diagnosis • Differentials: • IHD, valvular heart disease, pulmonary disease • Echo, CMRI +/- angiogram can be useful in distinguishing • Echo: LV dilation, more spheroidal shape, RWMAs, usually global systolic dysfunction, can be focal. +/- pericardial effusion. • CMRI – inflammation, hyperaemia, oedema, necrosis, scar, systolic dysfunction • Definitive Diagnosis • Pathological diagnosis • Endomyocardial biopsy – histology “ Dallas Criteria” • Immunohistochemical stains, PCR for viral genomes
Management: • Treat as ACS if features are indistinguishable – troponin elevation, ischaemic changes on ECG, risk factors for CAD or history of same. • Urgent Echo if large effusion or compromise • CHF • Usual therapies: diuresis, fluid and Na restriction, ACEi, B-blockers. • May require balloon pump • Arrhythmias • Need monitoring, • TachyC can precipitate CHF – amiodarone, cautious BB, CCB • BradyC pacing – usually only with temporary wire • Anticoagulation
Management: • Specific therapies: • Anti-virals: usually outside of treatment window – don't often see early myocarditis. • Immunosuppressive agents: Inflammation exceeds infection, effective in some animal studies but difficult to assess response in people due to rapid spontaneous recovery. Corticosteroids, cylcophosphamide, azathioprine – may exacerbate viral causes. • Immunoglobulin – may be useful • NOT NSAIDs • Cardiac transplant → chronic myocarditis with persistent CHF • Bed rest during acute phase – fevers and infective symptoms • Reduction in alcohol intake • Follow up 1-3 monthly with regular Echo
Prognosis • Mild cases unclear as only most unwell get EMB and diagnosis. • Dependent on cause • Fulminant myocarditis – much better prognosis, most return to normal LV systolic function. • Idiopathic Giant cell myocarditis usually fatal • Usually inflammation is self limiting without long term sequelae • Poorer prognosis if: • ECG: BBB, high degree AV block, Q waves • LVEF < 40% • Pulmonary hypertension