Download
1 / 26
330 likes | 1.06k Views
Femoral neck fractures. Re-written by: Daniel Habashi. Anatomy. Physeal closure at the age of 16 Neck-shaft angle 130 ° +/- 7 ° . Anteversion 10 degr +/- 7 degr Calcar femorale Posteromedial Dense plate of bone. Blood Supply.

E N D
Femoral neck fractures Re-written by: Daniel Habashi
Anatomy • Physeal closure at the age of 16 • Neck-shaft angle 130° +/- 7 ° . • Anteversion 10 degr +/- 7 degr • Calcarfemorale • Posteromedial • Dense plate of bone
Blood Supply • Greater fracture displacement = greater risk of vascular disruption to femoral head • Revascularization of the head • Intact vessels • Vascular ingrowths across the fracture site
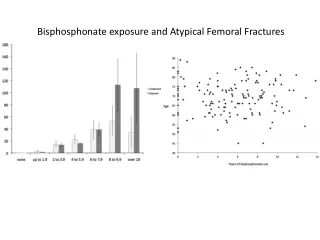
Epidemiology • 250 thousand hip fractures annually
Classification • Pauwels • Angle describes vertical shear vector • Type 1 = 30° • Type 2 = 50° • Type 3 = 70 °
Classification • Garden (1961) • I • Valgus impacted or incomplete • II • Complete non displaced • III • Complete partial displacement • IV complete full displacement • ** portends risk of AVN and nonunion
Classification • Functional classification • Stable • Impacted Garden I • Non-displaced Garden II • Unstable • Displaced Garden III and IV
Treatment • Non-Operative • Very limited role • Activity modification • Skeletal traction • Operative • ORIF • Hemiarthroplasty • Total hip replacement
Decision making variables • Patient characteristics • Young (under 65) • High energy injuries • Often multi-trauma • High Pauwels angle (vertical shear pattern) • Elderly • Lower energy injury • Comorbidities • Pre-existing hip disease • Fracture characteristics • Stable • Unstable
Young patients • Non-displaced fractures • At risk for secondary displacement • Urgent ORIF recommended OPEN REDUCTION INTERNAL FIXATION • Displaced fractures • Patients native femoral head best • AVN related to duration and degree of displacement • Irreversible cell death after 6-12 hours • Emergent ORIF recommended
Pre-operative considerations • Regional vs general anesthesia • Mortality / long term outcome • No difference
Pre-operative considerations • Surgical timing • Surgical delay for medical clearance in relatively healthy patients probably not warranted • Increased mortality, complications, length of stay • Surgical delay up to 72 hours for medical stabilization warranted in unhealthy patients
Non-displaced fractures • ORIF – standard of care • Predictable healing • Nonunion under 5% • Minimal complications • AVN under 8% • Infection under 5% • Relatively quick procedure • Minimal blood loss • Early mobilization • Unrestricted weight bearing with assistive device PRN
Approach for open reduction • SMITH-PETERSON • Anterior approach • Best for transcervical
Sliding compression screw fixation • Compression hip screws • Sacrifices large amount of bone • May injure blood supply • Biomechanically superior in cadavers • Anti-rotation screw often needed • Increased cost and operative time • No clinical advantage over parallel screws • May have role in high energy / vertical shear fractures
HemiarthroplastyUnipolar vs. Bipolar • Bipolar theoretical advantages • Lower dislocation rate • Less acetabular wear / protrusio • Less pain • More motion
Hemiarthroplasty cemented vs. non-cemented • Cement (PMMA) • Improved mobility, function, walking aids • Most studies show no difference in morbidity / mortality • Sudden intra-op cardiac death risk slightly increased:
Cemented vs. non-cemented • Conclusion • Cement gives better results • Function • Mobility • Implant stability • Pain • Cost-effective • Low risk of sudden cardiac death • Use cement with caution
Pre-operative considerations • Surgical approach • Posterior approach to hip • 60% higher short-term mortality vs. anterior • Dislocation rate • No significant difference
ORIF or Replacement • Prospective, randomized study ORIF vs. cemented bipolar hemi vs. THA • Ambulatory patients > 60 years of age
Stress Fractures • Patient population • Females 4-10 times more likely
Stress fractures • Clinical presentation • Activity weight bearing related • Anterior groin pain • Limited ROM at extremes • +/- antalgic gait • Must evaluate back, knee, contralateral hip
Stress fractures • Imaging • Plain radiographs are negative in up to 66% • Bone scan • Sensitivity 93-100% • Specificity 76-95% • MRI 100% sensitive / specific • Also differentiates synovitis, etc
Stress fractures - complications • Tension sided and compression sided fx’s over 50% treated non-operatively • Varusmalunion
Femoral neck nonunion • Definition: not healed by one year • 0-5%