Download
1 / 13
130 likes | 236 Views
Quantifying Health Benefits with Local Scale Air Quality Modeling. Presentation to CMAS October 7 th , 2008 Bryan Hubbell, Karen Wesson and Neal Fann U.S. EPA Jonathan I. Levy Harvard School of Public Health. Overview.

E N D
Quantifying Health Benefits with Local Scale Air Quality Modeling Presentation to CMAS October 7th, 2008 Bryan Hubbell, Karen Wesson and Neal Fann U.S. EPA Jonathan I. Levy Harvard School of Public Health
Overview • Summarize how we estimate human health benefits with local air quality modeling data • The basic steps in an Environmental Benefits Mapping and Analysis Program (BenMAP) benefits analysis • Matching the health data with the scale of the air quality data • Understand how local-scale benefits are influenced by: • Resolution of exposure estimates • Scale of baseline incidence rates • Geographic specificity of health impact functions • Discuss directions for future research
Step One: Derive Health Impact Functions from Epidemiology Literature Epidemiology Study Ln(y) = Ln(B) + ß(PM) Incidence (log scale) Ln(B) ∆ Y = Yo (1-e -ß∆ PM) * Pop Health impact function PM concentration Yo – Baseline Incidence ß - Effect estimate Pop – Exposed population
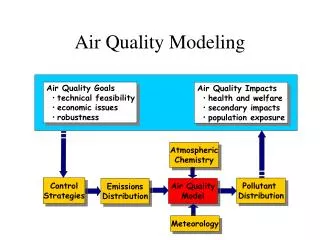
Step Two: Apply the Health Impact Function to Estimate Benefits Baseline air quality Post-policy air quality Estimate air quality change Estimate population exposure Health Benefits ß Apply the effect estimate to quantify health impacts Match exposure with baseline incidence rate
National-Scale Modeling Calls for Coarse-Scale Health Inputs Coarse-scale air quality modeling Coarse-scale population exposure Regional or national-scale Baseline incidence and ß estimate Regional or national Incidence count
Local-Scale Modeling Calls for Location-Specific Health Inputs Fine-scale air quality modeling Fine-scale population exposure Regional or national-scale Baseline incidence and ß estimate Local Incidence count
Comparing Population-Weighted Air Quality Changes at 12km and 1km Air quality change * Population at 12km Air quality change * Population at 1km
Exposure Estimates Sensitive to Air Quality Modeling Scale • PM2.5 Population-weighted air quality change highly variable • 12km: -0.037 µg/m3 • 1km: -0.715 µg/m3 • Summary conclusions: • 12km and 1km population exposure different • Population exposure affected by proximity of population centers to changes in grid-level air quality
Assessing the Importance of Baseline Incidence Rate Scale • We calculate health impacts relative to some baseline rate • Local analysis calls for local incidence rates • Michigan DEQ provided ZIP-level rates for: • Respiratory hospitalizations • Asthma • Chronic Lung Disease • Pneumonia • Non-fatal heart attacks • Acute Bronchitis • Chronic Bronchitis
Chronic Bronchitis Rate Varies by Age and Location in Detroit
The Level and Distribution of Avoided Chronic Bronchitis Cases is Sensitive to the Incidence Rate Change in chronic bronchitis using national incidence rate Change in chronic bronchitis using Detroit incidence rate
O3 Benefits are Sensitive to the Scale of the Health Impact Function Original Bell et al. (2004) mortality estimate Detroit-specific Bell et al. (2004) mortality estimate
Local Health Impact Analyses are Data-Intensive • How best can we use local-scale air quality modeling when we lack local: • Health impact functions? • Incidence rates? • Do you use local concentration-response functions when: • They exhibit poor statistical power due to small population sizes? • Are sometimes negative? • They lack statistical significance? • At what scale do you violate the fundamental assumptions of epidemiology study?