Download
1 / 92
950 likes | 1.2k Views
SWINE FLU. What is it? What can I do? An Indian perspective! Dr. T.R.Chandrashekar Director critical care Dr. N.K. RAGHURAM

E N D
SWINE FLU What is it? What can I do? An Indian perspective! Dr. T.R.Chandrashekar Director critical care Dr. N.K. RAGHURAM Fellow in CCM K.R HOSPITAL Bengaluru, India
What do we do? • We have recorded 24 deaths • We have no Medical guidelines of do’s and don'ts • Young people are dying-is their a pattern • Can we pick them early before they turn sick? • Testing in few center’s-takes 4 days to get results • Do we start Tamiflu in all suspected cases? • Deterioration is occurring on 4th day and death on 7th or 8th day • Where do we stand?
CHALLENGES WE FACE • Recognition of disease • Not to forget chikungunya & dengue • Difficulty in Confirmation of disease • Self protection • Protection of people around us • Notification • To know more ; Are we facing the pandemic?
Scenario • Admitted suspected Patient (symptoms+ travel history) • Sample sent for PCR • Reported positive H1N1 • What to do for patient relatives& hosp staff who are exposed Patient with hemodynamic compromise & respiratory difficulty Need for intubation-To proceed & then send sample for PCR What to do meanwhile Is it necessary to test all doctors & staff
Enigmatic questions • Should we close the hospital & fumigate? • What to do for other patients next to the case • Should we send all suspected cases to referral hospital
Subsequent challenges • Recognising in OPD- identify flu symptoms, travel history, clinical signs of hemodynamic derangement &pneumonia/ALI/ARDS • Proper referral to institutions handling cases • Isolation rooms, Use of masks Hand wash • Ventilatory management
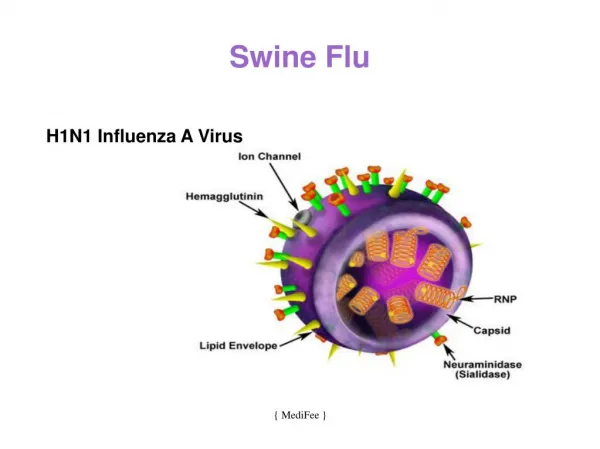
Influenza At A Glance • Influenza, commonly called "the flu," is caused by viruses that infect the respiratory tract. • Influenza viruses are divided into three types, designated A, B, and C.
VIRAL VARIANTS • INFLUENZA A VIRUS • Swine Human Avian • H1N2 H1N1(pandemics) H5N1 • H3N1 H3N2 (rare) • H3N2
QUADRUPLE REASSORTMENT GENETICS • Human swine • Avian swine H1N1
EARTH LIVING SPACE FOR ALL • Epidemic: An increase in disease above what is normally expected • Pandemic: A worldwide epidemic • A pandemic begins when: there is person-to-person sustained transmission on multiple continents
HISTORY • In the 20th century there have been three influenza pandemics in 1918, 1957 and 1968.
WHO • April 24: H1N1 first disease outbreak notice. • April 25:WHO Director General declares a formal “Public health emergency of international concern” • April 27:“containment of the outbreak is not feasible” pandemic alert raised from phase 3 to phase 4. • April 29:phase 4 to phase 5. • June 11:phase 5 to phase 6.
The World Health Organization uses a six stage phase for alerting the general public to an outbreak • Phase 1 – animal to animal transmission. • Phase 2 – an animal influenza virus is capable of human infection. • Phase 3 - small outbreaks among close populations but not through human to human contact.
Phase 4 -Human to human transmission • Phase 5 - spread across two countries or more in one of the WHO regions (continents). • Phase 6 – spread across two countries or more in one of the WHO regions plus spread to another WHO region.
Global pandemic • W.H.O. identifies the following six epidemiological sub-regions. • - African Region • - Eastern Mediterranean Region • - European Region • - Region of the Americas • - South-East Asian Region • - Western Pacific Region
EPIDEMIOLOGY • Incubation period- 1-7 days • Transmission PRIMARY CASE –direct contact with pigs SECONDARY CASES sneezing, coughing resp droplets body fluids(diarroeal stool) contact surfaces
This virus is not transmitted from eating pork or pork products • Contagiousness: 1 day onset of symptoms 7 days Children are contagious for longer periods. . Majority of pts were previously healthy. Clinical course mild in PCR negative influenza.
Majority of pts were previously healthy. • Clinical course mild in PCR negative influenza. • Pregnant women — Increased rates of spontaneous abortion and preterm birth • Patients with swine flu were found to have increased incidence of cardiovascular & cerebrovascular events.
Can I get infected with this new H1N1 virus from eating or preparing pork? • No. H1N1 viruses are not spread by food. You cannot get this new HIN1 virus from eating pork or pork products. Eating properly handled and cooked pork products is safe.
Is there a risk from drinking water? • Recent studies have demonstrated that free chlorine levels typically used in drinking water treatment are adequate to inactivate highly pathogenic H5N1 avian influenza. It is likely that other influenza viruses such as novel H1N1 would also be similarly inactivated by chlorination.
What kills influenza virus? • Influenza virus is destroyed by heat (167-212°F [75-100°C]). In addition, several chemical germicides, including chlorine, hydrogen peroxide, detergents (soap), iodophors (iodine-based antiseptics), and alcohols
Risk factors • COPD • Immunocompromised state • DM • Pregnancy • Cardiac disease • Obesity
DEFINITIONS • Influenza-like illness (ILI) is defined as fever (temperature of 100ºF [37.8ºC] or greater) with cough or sore throat in the absence of a known cause other than influenza
Case Definitions By CDC • A confirmed case acute febrile respiratory illness with laboratory-confirmed H1N1 influenza A virus detection by real-time reverse transcriptase (RT)-PCR or culture. • A probable case acute febrile respiratory illness who is positive for influenza A, but negative for H1 and H3 by RT-PCR
A suspected case acute febrile respiratory illness who: • - Develops symptoms within seven days of close contact with a person who is a confirmed case of H1N1 influenza A virus infection or • - Develops symptoms within seven days of travel or resides in a community where there are one or more confirmed H1N1 influenza A cases
Close contacts • Having cared for or lived with a person • setting where there was a high likelihood of contact with respiratory droplets and/or bodily fluids • Having had close contact (kissing, embracing, sharing eating or drinking utensils, physical examination, or any other contact likely to result in exposure to respiratory droplets)
Mexican data • Influenza-like illness or respiratory symptoms developed in 22 of 190 health care workers • These 22 workers received oseltamivir • for 5 days and were sent home for 3 to 7 days. They had mild-to-moderate disease, and none required hospitalization nejm.org august 13, 2009
Preventive measures taken in Mexican hospitals • After infection-control measures were strictly enforced — with patients confined and isolated in three hospital areas and N95 masks • Separate respirators used in addition to goggles, gowns, and gloves, as well as liberal use of gel-alcohol hand sanitizer — no more health care workers had influenza-like illness, nejm.org august 13, 2009
AGE SHIFTS IN MORTALITY • Concept of “original antigenic sin,”by Francis - immune response is greatest to antigens to which first exposure occurred in childhood. • Persons born before 1957 who were exposed in childhood to influenza A (H1N1) viruses might be better protected against this viral subtype than those who were first exposed to other influenza A subtypes, H2N2 and H3N2, at a later date .
During the early phase of this epidemic, the rapid identification of persons who are likely to have severe disease, as compared with those who are likely to have mild disease, can guide epidemic or pandemic response strategies.
Specimens • Nasopharyngeal swab, nasal swab, throat swab, combined oropharyngeal/ nasopharyngeal swab, or nasal aspirate • Swabs with a synthetic tip (eg, polyester or Dacron) and an aluminum or plastic shaft should be used. Swabs with cotton tips and wooden shafts are not recommended. • The collection vial in which the swab is placed should contain 1 to 3 mL of viral transport media.
Respiratory specimen should be collected within 4 to 5 days of illness. Specimens should be placed in viral transport media and placed on ice (4ºC) or refrigerated immediately for transportation to the laboratory
QUIDEL RT PCR CULTURE DFA/IFA DIAGNOSTIC TESTS
LAB TESTS • Real time RT PCR-confirmatory • culture is usually too slow to help guide clinical management. A negative viral culture does not exclude pandemic H1N1 influenza A infection. • Rapid antigen tests — evaluation of patients suspected of having influenza, but results should be interpreted with caution the QuickVue Influenza A+B (Quidel) assay (sensitivity 51 percent specificity 99 percent)
Rapid influenza antigen tests & Direct or indirect immunofluorescent antibody testing (DFA or IFA) can distinguish between influenza A and B but negative test does not exclude infection.
Whom to test • Testing for pandemic H1N1 influenza A should be considered in individuals with an acute febrile respiratory illness ( temperature of 100ºF or higher and recent onset of at least one of the following: rhinorrhea, nasal congestion, sore throat, or cough) or sepsis-like syndrome
Priority for testing should be given to : Those who require hospitalization and Those who are at high risk for severe complications No testing if illness is mild or the person resides in an area with confirmed cases Recommended test for suspected cases is real-time reverse transcriptase (RT)-PCR for influenza A, B, H1, and H3
CLINICAL FEATURES Vomiting or diarrhea (not typical for influenza but reported by recent cases of swine influenza infection)