Download
1 / 29
290 likes | 469 Views
Anti-infectives. Parasitology. Parasitology Schistosomiasis: is caused by S. haematobium &/or S. mansoni & causes liver cirrhosis . This can be treated by praziquental .

E N D
Anti-infectives Parasitology
Parasitology • Schistosomiasis: is caused by S. haematobium &/or S. mansoni & causes liver cirrhosis. This can be treated by praziquental. • Scabies is an exo-parasite caused by mites. It can be eradicated by gamma-benzene hexachloride or benzyl benzoate or Sulphur ointment 10%. • Drugs used in the treatment & prophylaxis of Malaria include: • Chloroquine (Aralen) – Pyrimethamine • Quinine (in treatment only) – Primaquine • To be given one weak before exposure & 4-6 weeks after leaving the endemic area. • Primaquine is the most effective & least toxic of the 8-amino-quinolone group. • Drug of choice for prophylaxis of malaria: is Chloroquine. • Pyrimethamine ( usually with sulfadoxine), Fansidar, & Primaquine are only used in treating chloroquine resistant cases. • Quinine: (an optical isomer of Quinidine) is only used in treatment. Available as the SO4 (oral) or HCl (IV) salts. • Tape worms: Both Beef worm (Tinia saginata) & Pork worm (Tinia solium)are treated by either Quinacrine or Niclosamide. • Quinacrine: should not be used in the treatment of tape worm in patients who have a history of psoriasis, psychosis, elderly or those with liver disease. • Niclosamide: is an anthelmintic drug, most effective against beef & pork tape worms. • Hook worm (Ancylostoma duodenalis): is a parasite capable of entering the body through intact skin. It is treated with thiobendazole or mebendazole. • Thiobendazole (Mintezol): is an anthelmintic drug, which is effective against multiple infestations, e.g. whip worm, cat & dog hook worm, T. trichura, & strongyloids (thread worm).
Anti-infectives Anti-microbial
General • Thermal Death Point: is the temperature at which all bacteria of a given species are killed after 10 min of exposure to heat. • Dry heat sterilization: this type of sterilization is an oxidation process. • Mineral oils are sterilized by dry heat process. • Gas sterilization (Alkylation): is used for sterilization of some substances (plastic). Ethylene oxide is the agent used in the process. • How to kill spores: by moist heat at 100oC for 15 min for 3 successive days. Alternatively, autoclaving at 121oC for 20 min. • Globigu: is a variety of Staphylococci that is resistant to heat. • Acid fast bacteria: are a special type of bacteria (e.g. Mycobacterium) which differs from other types of bacteria in: • Containing high conc. of fatty acids. • Presence of mycolic acids & fatty substances. • Drug fastness: Mutational forms of the original bacterial strains usually appear due to exposure to sub-clinical (sub-therapeutic) doses of the drug. • Pyoderma: is a pus forming skin infection (pyo = pus). • Bubble Point Test: is used to check leakage of bacterial filters. • Hepa filters: are used to remove particles from air. These are used in the laminar flow hood. • The pore size for bacterial filters is 0.22 nm. • A fomite: is a non-living material (e.g. needles, syringes) capable of transmitting infection. • Complications of corticosteroids therapy: • Increased susceptibility to infection (immuno-suppression). • Masking symptoms of infection. • Spread (dissemination) of local infection. • Negric bodies: these are spherical, eosinophilic inclusion bodies, found in nerve cells of rabid animals or humans. They are formed due to allergic reaction. • Granulomas are caused by M. tuberculosis. • Agranulomas are caused by M. lepre.
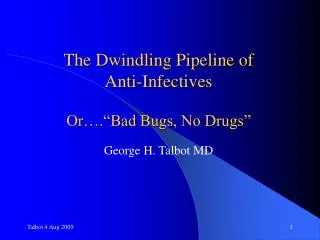
c d Log Bacterial Number b a Time (hrs) General • Growth sequence of bacterial cells: When a given bacteria is seeded on a suitable medium, at a suitabletemp., its growth will follow a definite course. The growth curve can be divided into 4 phases: a. The lag phase. b. The logarithmic phase. c. The stationary phase. d. The phase of decline. • Conjunctivitis may be bacterial, viral, fungal, parasitic, or allergic. • Bacterial conjunctivitis is caused by S. aureus, S. pneumoniae & Hemophilus spp. • In Canada, Chlamydia trachomatis is often isolated from conjunctiva of children, ttt AgNO3 • Eye infections in Canada: the most common causative organism is P. aeruginosa. These are treated by gentamycin eye drops & / or ointment. • In encephalitis, gentamycin is the most useful to treat infections caused by susceptible P. aeruginosa strains (carbenicillin can be used but resistance develops rapidly). • Neonatal Meningitis in Canada:the most common causative organism is H. influenzae. • Causative pathogens in meningitis: Neonatal (0-1 month) E. coli, Stept B, Lysteria, or Herps simplex 1month – 4 yrs H. influenzae Adults S. pneumoniae / N. meningitidis. • In meningococcal encephalitis:tetracycline, chloramphenicol, or sulphonamides can be used as they pass BBB. Streptomycin can pass the inflamed meninges only, it does not pass the normal meninges. Crystalline penicillin can be used but has to be given intra-thecal. • Middle ear infections are caused by: • S. pneumoniae, H. influenzae in children • S. aureus, hemolytic streptococci in adults • S. aureus, E. coli in neonates • Generally, S. pneumoniae & H. influenzae are the most common isolates in AOM. Less frequently isolated pathogens are GABHS, M. catarrhalis & S. aureus. G –ve (P. aeruginosa, E. coli, K. pneumoniae & Proteus) are rarely isolated. Clostridium is never found in ear. • Sinusitis & mastaditis are caused by S. pneumoniae & H. influenzae • In cases of mixed infections: we can use a combination of antibiotics (sometimes a bactericidal + bacteriostatic). • INH, tetracyclines & erythromycin may result in hepatic toxicity & GIT problems. • Sulfaisoxazole, naladixic acid, primaquine & probenecid may result in hemolytic anemia in patients with glucose-6-phosphate dehydrogenase deficiency (Favism).
The Bacterial Cell Wall: • In G +ve bacteria: the cell wall consists of peptidoglycan & teichoic acid. • In G -ve bacteria: the cell wall consists of peptidoglycan, lipoprotein layer & lipo-polysaccharide + phospholipid outer membrane. • The Gram Stain: the basis of the differential gram stain is the cell wall structure. • The procedure begins with the application of a basic dye, crystal violet. • A solution of iodine is then applied. At this point all bacterial cells will be stained blue. • Cells are then treated (washed) with alcohol. • G +ve cells will retain the crystal violet – iodine complex & remain blue. • G –ve cells will be completely decolorized. • The last step is applying a counter stain (e.g. the red dye Safranin) so that G –ve cells will take a contrasting color. • G +ve retains the dye (gentian violet) because of teichoic acid. • G -ve does not retain the dye because of the lipid membrane. • G +ve pathogensaexotoxins G –ve pathogensa endotoxins • Eukaryotic & Prokaryotic Cell Structure: Eukaryotic (Fungi & Yeast) Prokaryotic (Bacteria) Cell Structure More complex inside More complex outside Nucleus Is bounded by a membrane that is Absence of nuclear membrane continuous with endoplasmic reticulum & true nucleus [1 super-coiled DNA strand (nucleoid)] Ribo/Chromosomes: not distinguishable / on reticulum Only 1 chromosome / free Cytoplasm Presence of endoplasmic reticulum, Absence of mitochondria Golgi apparatus & mitochondria. & membranous inclusions Mobile (plasmids, reticulum). Immobile Protein synthesis 80 S ribosome 70 S ribosome Reproduction Mitosis Asexually (binary fission) Respiration Site Mitochondria Cytoplasmic membrane Locomotion Ameboid / Flagellae Flagellae / Cilia Cell size Large Small Cell envelopeConsists of 3 layers: Multilayered: a. Cytoplasmic membrane a. Cytoplasmic membrane b. Peptidoglycan layer absent b. Peptidoglycan layer c. Outer membrane c. Variable outer layer (capsule) d. Variable outer layer (capsule) • Plasmids: are genetic elements that carry antibiotic resistance genes of a micro-organism. • A Mordant: is a substance that fixes bacterial stain & becomes permanent (to differentiate G +ve bacteria, which retains the dye, from G –ve bacteria that does not retain the dye).
Bacterial Infections Gram-positive Cocci Infections: • Scarlet fever: is caused by S. pyogenes & is characterized by fever, rash & strawberry tongue; It is treated by sulfadiazine & penicillin (less commonly with chloramphenicol). • Rheumatic fever: is an immunological reaction to repeated infections by GABHS infections. It causes cardiac valve damage. • S. viridans (a hemolytic streptococci): involved in sub-acute bacterial endocarditis & pyorrhea alveolaris & UTIs. It can be treated with a long course of penicillin V. During the infection, fever tends to peak during night & early morning hours (10 pm – 6 am). • Postulant ear boils are usually caused by staphylococci in the anterior portion of the external auditory canal. • Acute toxic shock syndrome: is caused by tampons. Symptoms include sudden high fever, headache, sore throat, vomiting, diarrhea (flu-like syndrome). The causative pathogen is S. aureus. It occurs both in men & women (esp. young females) Gram-negative Cocci: • Neiserria gonorrhea: the drug of choice for urethral & urogenital gonorrhea is penicillin + probenicid or tetracyclin. Spectinomycin is an alternative in penicillin allergic patients. Gram-positive bacilli infections • Diphtheria is caused by Corynobacterium diphtheria & can be treated by benzyl penicillin or erythromycin. • The diphtheria exotoxin causes laryngeal obstruction. • Schick’s test for diphtheria:ID injection of diphtheria toxin (0.1 ml) in the forearm. A +ve reaction means susceptible (not immune) to diphtheria. The reaction consists of local redness after 24-36 hrs & persists for 4-5 days. • The Genus Clostridium: these are anaerobic, spore-forming G +ve bacilli, resistant to heat, & capable of producing exotoxins. They can be subdivided into: • Clostridium difficile: pseudomembraneous colitis, treated with vancomycin. • Clostridium botulinum: botulinum exotoxins botulism (food poisoning), usually associated with anaerobic growth of the organism in improperly canned food (meat & non-acidic vegetables); it is destroyed by boiling for 10 min. The M.O is also found in soil & GIT of domestic animals. Botulism is treated by polyvalent (bivalent) anti-toxin. • Clostridium tetani: tetanus, treated with vancomycin IV. • Clostridium preferengens (C. welshii): Gas gangrene whichspreads rapidly & has a necrotizing effect. The organism is capable of devitalizing living tissue.
Gram-negative Bacilli Infections • Neonatal meningitis is caused by H. influenzae. • E. coli:is the most common causative pathogen in UTIs. • Pseudomonas sp. are sensitive to aminoglycosides, carbenicillin (but resistance develops). They are generally not sensitive to cephalosporins (except ceftazidime & cefepime). • Salmonella typhi: is the causative pathogen of typhoid fever. The most common location of the organism in a typhoid carrier is the gall bladder ( the UT may be involved). In culture media, it does not ferment glucose nor sucrose & does not produce gas. • Shigella: is the causative organism in bacillary dysentery. It is generally classified as non-lactose fermenter of the gp. Enterobacteriacae (also Salmonella), & the subdivided further according to the antigen properties. • Cholera: caused by Vibrio cholera (Comma bacillus, Koch’s bacillus), produces endotoxin. • Chlamydia trachomatis: constitutes part of the normal flora of the nose & throat & less commonly of the vaginal cervix. It is the causative agent of trachoma including conjunctivitis & urethritis. Infants may contract chlamydial eye infections during birth, from a maternal cervical infection (treated by AgNO3 eye wash). • Brucellosis (Malta fever): is characterized by fluctuating temperature (undulant fever) & is treated by a combination of tetracycline + streptomycin or with rifampecin. • Plague is caused by Yersina or Pasturella pestis. It is transmitted from rats (carrier) by flees. • Tularemia: is transmitted by a bite of infected flees or ticks, the reservoir animals are rodents (rats, rabbits, …) & semi-aquatic mammals (musk rats). It is treated by TC + streptomycin. Mycobacterium infections • Tuberculosis: caused by Mycobacterium tuberculosis (G +ve bacilli), INH in prophylaxis. • Tuberculin test: is based on the fact that small amount of tuberculin, if injected in a tuberculous subject will produce a local swelling at the site of injection. • Mantoux test: is the most accurate & sensitive type of tuberculin test. • Leprosy: is caused by Mycobacterium leprae & is treated with Dapson. Spirochetes • Syphilis: is caused by Treponema pallidium (anaerobic rods / spirochetes) & can be treated by benzyl penicillin. It is characterized by production of chancre. • Trench Mouth: is caused by Borrelia vincenti (spirochetes), normally found in the mouth with Borrelia buccalis. • Leptospira icterohaemorrhagia: is the etiological agent of leptospirosis (Weil’s disease) & cause infective jaundice in humans.
Viral & Rickettsial Infections:These differ from bacteria in that they do not survive outside a living tissue, while bacteria can grow on synthetic media. • Rocky mountain spotted fever: is caused by Rickettsia rickettsi transmitted by ticks to man & animals, & treated with chloramphenicol (CM) or Tetracyclines (TCs). • Endemic Typhus: caused by R. prowazikii & transmitted by lice; treated by CM or TCs. • Tetracyclines: are the most effective agents against rikettsial infections. • Mumps: the incubation period of mumps in humans is 14 – 21 days. • Koplick’s spots: are white spots on mucous membranes & are associated with measles. • Passive immunization of contact children is made using gamma globulin. • Biavax II: is a mixture of living mumps & rubella viruses used for immunization (vaccine). • Hepatitis A: transmitted by food/water, droplet, direct personal contact, oral/fecal routes. • Hepatitis B is transmitted either through: Direct contact with blood & blood products or Sexual transmission • Interferon: is a glycopeptide complex which inhibits viral replication. • Herpes simplex is a viral infection of the eyelid & conjunctiva. It is treated by iodoxuridine eye ointment or drops (never given orally as it affects the DNA). It may also infect: • Oral cavity (through kissing) stomatitis. • Eyes (through contamination) kerato-conjunctivitis. • Penis & vulva (sexual intercourse) vesicular lesions (Herpes genitalis) associated with cold sores or oral herpes simplex. • Fingers (through touching oral secretions) paranychia. • Skin (through droplet infection) vesicular lesions (chicken pox). • Herpes Zoster (schingle’s disease): is a neurotropic virus, transmitted through contact or droplet infection acute CNS infection (posterior root ganglion) characterized by formation of very painful vesicular eruptions in the area of the affected nerve. • Epstein-Barr Virus (EB virus): (Lysteria monocytogenes) • Is a herpes virus mononucleosis (# No of monocytes above normal). • Rabies: a viral infection characterized by CNS involvement paralysis & finally death. It may be communicated to man through the bite of a rabid animal (saliva of a dog). • Iodoxuridine (Stoxil): is an antimetabolite that inhibits replication of viral DNA. It has greater selectivity for viral (rather than host) DNA. It is the drug of choice for treating Herpes Simplex of the eye lid & conjunctivitis (also for simplex kerotitis). • Vidrabine (Vira A): is an antiviral believed to inhibit viral replication & is effective against herpes simplex eye infections. • Amantadine (Symmetrel): is a tri-cyclic antiviral (for influenza A) • Besides, it can be used to treat parkinsonism (it stimulates the release of dopamine).
Fungal Infections • Ring worm is a dermatophyte. Dermatophytes cause: • Tinea capitis in the scalp. • Tinea pedis cause athlete's foot. • Tinea ungium in nails (onchomycosis). • Tinea cruris in the groin. • Treatment of dermatophytes (ring worm): • Tolnaftate used in to treat tinea pedis as a dusting powder &/or cream. It is not effective in candidiasis (only in dermatophytes). • Grisofulvin (only in dermatophytes). [ Also used to treat gout ]. • Clotrimazol(Canesten) can also be used in treatment of candidiasis. • Miconazol (Daktarin) can also be used in treatment of candidiasis. • Ketonazol (Nizoral) can also be used in treatment of candidiasis. • Econazol can also be used in treatment of candidiasis. • Meconazol: is used to treatcoccidio-mycosis & vaginally to control monilial infections. • Nystatin & Natamycin are only used to treat candidiasis but not dermatophytes. • Candicidin (Candeptin): is an antibiotic with a good antifungal action specially against vaginal candidiasis. • Amphotrecin B: (obtained from streptomyces nodosus). It is related to aminoglycosides. It acts on the cell membrane & is used to treat systemic fungal infections & deep mycosis. • Thrush is an inflammation of the buccal cavity caused by Candida albicans & is treated by nystatin. • Barbiturates (microsomal enzyme inducers) $ the antifungal activity of grisofulvin. Protozoal Infections • Trichomonas vaginalis is a flagellated protozoa, the causative agent for vaginitis. It is a sexually transmitted disease that is treated by metronidazole vaginal suppositories after menstruation. The normal pH of the vagina is 4.5 – 5. However during menstruation it increases causing symptoms (of vaginitis) to appear. • Metronidazole (Flagyl): beside its anaerobic activity (can be used in clostridium deficile), it is effective in amebiasis, giardiasis & trichomonas vaginalis. However it is not effective as an antifungal. • Emetine HCl: has a direct lethal action on amebiasis.
Classification of Antibiotics • Cephalosporins: similar to broad spectrum penicillins but they are more stable to penicillinases, thus they are used instead of penicillins in S.aureus infections. • Macrolides: These are the drugs of choice in patients with: d Penicillin hypersensitivity dM. pneumoniaed Legionaries disease • Erythromycin can be used during pregnancy. • The oesteolate salt of erythromycin has higher blood levels than the stearate salt, however it may cause cholestasis (since the erythromycin is excreted hepatically). • It is a good choice in patients with renal impairment. • Erythromycin oestolate: causes reversible cholestatic hepatitis with fever & jaundice (a hypersensitivity reaction to the oestolate salt, thus the stearate salt is preferable). • Tetracyclines: These are bacteriostatic antibiotics. • They inhibit protein synthesis in the bacterial cell. • Most commonly used in patients with mixed infections (Ricketsial). • All tetracyclines suffer cross-sensitivity & cross-resistance. • Long-acting tetracyclines include Doxycycline (Vibramycin) & Minocycline (Minocyn), used in RTIs. • Tetracyclines have the following adverse effects: d GIT disturbances d Photosensitivity d Fanconi’s syndrome: characterized by: nausea, vomiting, polyurea, acidosis. It results from the administration of expired (out-dated) tetracyclines. d Tooth discoloration: In children as a result of complex formation with Ca++. • Minocycline (Minocyn): is a long acting tetracycline used against resistant staph. • Minocycline & Doxycycline (Vibramycin): have much lower renal clearance rates than tetracycline & are not effective in UTIs (Tetracycline HCl can be used in UTIs). • Chloramphenicol: These are bacteriostatic antibiotics. • They inhibit protein synthesis in the bacterial cell. • Most valuable in treatment of G +ve & G -ve infections (Salmonella, Rickettsia) & also against ampicillin-resistant H. influenzae. • Adverse effects: dBone-marrow depression & blood dyscrasis including agranulocytosis (most common) & idiosyncratic aplastic anemia (most fatal) d Gray baby syndrome (in infants & preterm babies): immaturity of drug metabol- izing enzymes (glucoronyl transferase) in infants excessive serum conc. of unconjugated chloramphenicol maintained for several days circulatory collapse
NH2 SO2NH – R • Lincomycin (Lincocin) & Clindamycin (Dalacin): These are macrolide type antibiotics. • There use is restricted to anaerobic infections. • They cause serious diarrhea & colitis (pseudomembranous colitis). • Vancomycin: This is a bactericidal antibiotic with excellent G +ve coverage. • It is the drug of choice for MRSA / MRSE; it is too toxic for routine use. • Administered IV, except in cases of pseudomembranous colitis, where it is given orally. • Sulfonamides: these are bacteriostatic drugs that $ bacterial growth through competing with PABA in folic acid synthesis (inhibit folic acid synthesis) (competitive antagonism). Folic acid is an essential co-enzyme in the bacterial cell for the synthesis of nucleotides. • Can pass BBB (i.e. diffuse in the CSF). • Converted in the body to the non-substitutedaromatic amino gp. to have useful antibiotic activity. • Effective against G –ve & G +ve bacteria. • Metabolized by acetylation of the p-amino gp. • Excreted through the kidney used in UTIs. • Side effects: Steven Johnson’s syndrome, Agranulocytosis, photosensitivity. dSuccinyl Sulfathiazole:is a sulfonamide that is not absorbed from the GIT, used to decrease intestinal bacteria. d The most successful sulphonamides are the alicyclic type. If substituted, they will be better absorbed. • Trimethoprim: is an enzyme inhibitor, inhibiting folate reductase enzyme prevents conversion of dihydro-folic acid to tetrahydro-folic (folinic acid) (essential for DNA synthesis in the bacterial cell). [Dihydro-folate reductase inhibitor]. • Co-trimoxazole (Bactrim / Septrin): is a combination of sulfamethoxazole + trimethoprim. • Synergism exists between sulphonamides & trimethoprim against many bacterial spp. • Aminoglycosides: inhibit protein synthesis (30 S ribosome) • Are not absorbed from GIT (might be given orally to act locally in GIT infections). • Are useful in serious infections (e.g. gentamycin is the most useful in encephalitis). • Cause dose dependent nephro-toxicity. • Cause dose dependent oto-toxicity (damage of 8th cranial nerve esp. with streptomycin). • May produce neuromuscular blockade (may enhance the neuromuscular blockade of skeletal muscle relaxants as succinylcholine & tubocurarine). • Drugs as gentamycin, kanamycin & tetracycline are excreted through the kidney by glomerular filtration. Carbenicillin is excreted by renal tubular secretion. • Quinolones: e.g. norfloxacin, ciprofloxacin, pefloxacin, cinoxacin, enoxacin, naladixic acid, oxalinic acid.
Mechanism of Action of Antibiotics • Inhibition of cell wall synthesis: These are bactericidal antibiotics. d Penicillins d Cephalosporins d Vancomycin d Bacitracin d Cycloserine d Carbapenems • Inhibition of cell membrane function: These are mostly antifungals. d Amphotrecin B d Polymexin B d Nystatin dPolyenesd Imidazoles dColistin • Inhibition of protein synthesis: d Tetracyclines (30 S) d Streptomycin (30 S) d Aminoglycosides (30 S) d Macrolides (50 S) d Lincomycins (50 S) d Chloramphenicol (50 S) • Inhibition of nucleic acid synthesis: d Quinolones d Actinomycin D d Clofazimine d Rifampicin d Grisiofulvin d Pyrimethamine • Inhibition of folic acid synthesis: d Sulfonamides d Trimethoprime d Dapson N.B: Sulfonamides inhibit bacterial growth through competitive antagonism.
CH – COO CH S CH2 H N R – CO S N O COO – R` CH COOH Classification of Penicillins • Acid-labile, Penicillinase-sensitive: d Crystalline P d Procaine P d Benzathine P (L.A.) d Ticarcillin d Carbanicillin • Acid-stable, Penicillinase-sensitive : d Ampicillin d Amoxicillin d Phenoxy methyl P (P-V) • Acid-labile, Penicillinase-stable: d Methicillin • Acid-stable, Penicillinase-stable : d Oxicillin d Cloxacillin d Dicloxacillin d Nafcillin N.B: All penicillins, & their analogues exhibit cross-sensitivity. • Unit of Penicillin: This is the reference standard. 1 unit penicillin = the antimicrobial activity of 0.6 mg of USP sodium penicillin G. • 500,000 units of penicillin G = 300 mg of penicillin, thus 1,600 units = 1 mg of penicillin. General Structure of Penicillin: • Substitution at R` affects the solubility • Salts are water soluble & can be given orally. • Esters (procaine / benzathine) are poorly soluble & must be given IM • Substitution at R affects the stability of the lactam ring • Acid-labile, Penicillinase-sensitive: d Benzyl penicillin R = d Carbanicillin R = ( a-carboxy-benzyl penicillin) d Ticarcillin R = N.B: Both Ticarcillin & Carbanicillin are broad spectrum (anti-pseudomonal) but are acid labile (no oral form) & penicillinase sensitive.
Cl Cl CONH CONH CONH CONH N N N CH3 CH3 CH3 Cl O O O OC2H5 CH CH NH2 NH2 HO – O – CH2 OCH3 OCH3 • Acid-stable, Penicillinase-sensitive: d Ampicillin R = ( a-amino-benzyl penicillin) d Amoxicillin R = ( p-hydroxy a-amino-benzyl penicillin) d Phenoxy methyl P (P-V) R = • Acid-labile, Penicillinase-stable: d Methicillin R = ( 2,6 dimethoxy phenyl penicillin) The side chain confers b-lactamase stability • Acid-stable, Penicillinase-stable : d Oxicillin R = d Cloxacillin R = d Dicloxacillin R = d Nafcillin R =
Penicillins are short acting: because of the high rate of tubular excretion. • Probenicid prolongs the action of penicillins. It prevents rapid excretion of penicillin in proximal tubules (by competition). • Both probenicid & penicillin are acids & are uricosuric agents. In low doses they $ tubular excretion of uric acid (competitive inhibition). However in higher doses they inhibit the re-absorption of uric acid, # its excretion, thus can be used in gout. • There are 3 types of hypersensitivity reactions to penicillin: • Immediate Reaction: occurs within 20 min. & cause anaphylactic shock. • Accelerated reaction: occurs within 30 – 48 hrs & cause urticaria & laryngeal edema. • Delayed reaction: occurs after 3 days & usually involves urticaria. • Patients allergic to penicillin may show cross-sensitivity to cephalosporins & other beta-lactams (they share the same beta-lactam ring). • 10 – 20% demonstrate positive Coomb’s test. • Penicilloyl polylysine: is the substance used for skin test for penicillin allergy. • Penicillium Crysogenum: is a mould used commercially for production of Penicillin G. • Non-specific vaginitis: the organism most commonly involved is Haemophilus. It is treated with ampicillin 500 mg q 6 hrs for 6 – 10 days. • Penicillins & cephalosporins: have no effect on mycoplasma because it has no cell wall. • Penicillin is hydrolyzed to penicilloic acid by the action of penicillinase enzyme. • Penicillinis not used in combination with erythromycin since both have similar spectra.
Immunity • Immunity can be classified as: • Active Immunity: is done by the administration of an antigen (which might be a toxoid or an attenuated or killed bacteria). The body will develop its own antibodies as a reaction to the injected antigen. Active immunity is of long duration. The following biologicals are used for active immunization: d Toxoid: e.g. tetanus. d Killed bacteria (bacterial antigen): e.g. cholera or diphtheria. d Live attenuated bacteria (bacterial vaccine): e.g. mumps or measles. d Multiple antigen preparations. • Passive Immunity: Supply of ready made antibodies e.g. human immune serum (antitoxin). This supplies rapid immunity but of short duration (2-3 weeks). Additionally, it may cause allergy (being prepared from animal serum) d Immune gamma-globulin: is administered IM providing passive immunity which lasts for 1 – 2 months (e.g. infective hepatitis, chicken pox, measles). d Antibodies in immunity: interact directly with, & neutralize toxins. N.B: toxins are used as diagnostics, e.g. Schick’s test for diphtheria. • Toxoids: these are obtained from culture filtrate of viable organisms & the exotoxins thus obtained are treated with formaldehyde. The toxoid (inactive toxin) is used for active immunization against some organisms. • Toxoids:d Are detoxicated toxins. d Are antigens. d Are available in precipitated or adsorbed forms. d Produce artificial active immunity. They need a booster dose in order to sustain immunity (e.g. tetanus every 10 years). • Antitoxins: these are antibodies produced against bacterial toxins (or other toxins e.g. scorpion or copra venoms). Antitoxins are usually bound to a globulin fraction of the animal from which they were prepared & taken. • Antitoxins are given: d IM or IV for therapeutic effects. d IM or SC for prophylaxis. • Endogenous vaccines: are prepared from the patient’s own micro-organisms. • Adsorption of vaccines / toxoids allows for slow release & prolongs the presence of antigen.
Opsonins: these are antibodies that unite with bacteria facilitating their phagocytosis by phagocytic cells. • Agglutinins: When an antibody unites with an antigen to form suspended particles. The suspended antigens clamp together to form visible aggregates. This phenomenon is called agglutination & the antibody is called agglutinin. • Precipitins: when an antibody unites with a colloidal solution of the corresponding antigen, a precipitate (or visible floccules) will be formed & the antibody is called precipitin. • Complement Fixation: when the antibody unites with the corresponding antigen in presence of a third nonspecific normal serum constituent known as complement. The antigen antibody complex will attract & fix (or deviate) the complement in some way. • Bacteriolysins: these are antibodies that cause bacterial lyses through the fixation of complement. • Bacteriotropines: these are antibodies that are not bactericidal, but they mobilize the body defense against bacteria; i.e. promote phagocytosis.
Active Immunity Toxoid (DPT) (Diphtheria, Pertusis, Tetanus) Toxoid (DPT) Killed bacteria Killed bacteria Attenuated bacteria (BCG) Attenuated viruses Trivalent orally (Sabin) Attenuated viruses (MMR) Killed virus Killed virus Killed virus (elderly & cardiac pts) Passive Immunity Antitoxin, Globin Anti-Tetanus Serum (ATS) Gamma-globulin Anti-rabies serum / immunoglobulin Anti-venom Organism Diphtheria Tetanus Pertusis Cholera T.B Poliomyelitis V Mumps, Measles & Rubella Rabies Hepatitis B Influenza Snake Bite • Small pox vaccine: is a killed vaccine. It is made by making a glycerol suspension of vesicles of vaccinated animals. • Yellow fever vaccine (D17 vaccine): is a living attenuated vaccine, provides immunization that lasts for less than 1 year. (Yellow fever is endemic in tropical climates). • Tetanus antitoxin: This should be given IM or SC & its effect lasts for 10 days. • Sabin vaccine (Polio): is a living attenuated vaccine used for immunization against polio virus. It has a pink color & is administered orally. It is superior to Salk vaccine. • Rubella = German measles • Rabies Vaccine: (semple vaccine or Cow pox). It is a killed vaccine & to ensure this it must be tested for being non-infectious in rabbits. • Immunization against rabies: Rabies immunoglobulin has the advantage of lower incidence of allergic reactions compared to anti-rabies serum. • Influenza vaccine is given during October & November. N.B: Typhoid fever is a bacterial infection. Viral infections include: polio, measles, mumps, rabies & influenza, …etc.
Peritonitis: caused by bacteroid fragilis (gm –ve anaerobe) treated with clindamycin, metronidazol, or Imipenem • Dental infection: caused by Streptococcus viridans, Group A streptococci; treated with benzyl penicillin, procaine penicillin, penicillin G, Amoxicillin • Community acquired UTI: caused by E. coli, treated with gentamycin • Traveler diarrhea: caused by E. coli, Salmonella, or Shigella; treated with doxycyclin – metronidazol or co-trimazol. It can be prevented by drinking boiled water, avoiding raw food ??????????????????????????????? • Pneumocystic Carinii: Fungal infection cause interstitial pt (causes pneumonitis in infected elders & AIDS patient) treated by septrin • Lymes Disease: caused by Spirocharts, transmitted by rodents and deer by ticks bits. Treated by tetracycline or ceftriaxone. • Pseudomembranous colitis: caused by Clostridium dificile, associated with the use of clindamycin, ampicillin, ciproflaxin; treated by vancomycin. • Aminoglycoside vestibular gentamycin auditory kanamycin , amikacin • Grisiovulvin inhibits the growth dermatophytes 3 – 6 months nail 3 – 6 weeks hair, skin • Oesteomyletis Amoxicillin Cefixime (cephalosporins) Penicillin /clindamycin /gentamycin • Otitis Media AcuteRecurrent Amoxicillin Amoxi/clav Pivampicillin Cefaclor Septra Azithromycin Pediozole or Septra • Meningitis (3-6 months) H. influenza ampicillin or Ceftriaxone (> 6 months or adult) S. pneumonia Penicillin G or Vancomycin Neisseria Penicillin G or Ceftriaxone • UTI (acute uncomplicated): 1) Septra 2) Nitrofurantoin 3) Norflox. 4) Amox./clav 5) Cephalosporin • Vaginitis: 1) Bacterial: grey discharge + bad odor treatment clindamycin 2) Candida: cheesy discharge treatment nystatin / miconazole or chlotrimazole 3) Trichomonas: bad odor + pruritis + nurul
Anti-bacterial Drugs: • Bactericidal: • Beta-lactams (penicillins & cephalosporins) inhibit cell wall synthesis • Aminoglycosides bind to ribosomes • Quinolones inhibit DNA gyrase • Bacteriostatic: • Sulphonamides inhibit folic acid synthesis • Tetracyclines bind to ribosomes • Azoles bind to DNA • Macrolides (erythromycin) bind to ribosome • Chloramphenicol: interferes with protein synthesis by ribosomes (mainly bacteriostatic but may be bactericidal # H. influenza, N. meningitides, bacteroides spp.) • Clindamycin: bind to bacterial ribosomes inhibits protein synthesis Anti-viral Drugs • Drugs that directly impair virus replication • Acyclovir (Zovirax) – Idoxuridine • Vidarabine – Amantadine • Zidovudine (Retrovir) – Ganciclovir • Drugs that modulate the host immune system • Interferons Antifungal Agents • Polyene antibiotics bind to cell membrane → leakage → death Amphotericin & Nystatin • Azoles A) Imidazoles: Interfere with fungal oxidative enzymes # H2O2, Interfere with cell wall?? • Ketoconazole Miconazole Clotrimazole • Isoconazole Tioconazole Econazole B) Triazoles: Damage fungal cell membrane: itraconazole, fluconazole • Others • Griseofulvin • flucytosine
Bacteria is characterized by the absence of: • Flagella c. Mitochondria • Neoclid d. Nucleus • Influenzae vaccine is: • Vaccine is from killed virus (for A & B but not C) • Vaccine is especially given to elderly & pts with heart disease • A new vaccine is developed each year • Period of infection is during the winter • Contains RNA • The most common organism in UTI is: • E. colib. S. pyogenes • The most common organism in neonatal eye infections is: • P. aeruginosab. S. aureus • The most common organism in neonatal conjunctivitis in Canada is: • Chlamydia tricmontosac. S. aureus • P. aeruginosa d. Neisseria spp. • Which organism is not found in the ear: • Clostridium b. S. pneumoniae • If you get a smear from the middle ear, you expect to find: • Clostridiumb. S. aureus c. E. coli • Metronidazole (Flagyl): • Can not be used as antifungal. • Not effective in gonorrhea. • Is used in the treatment of Trichomonas vaginalis • Is very potent in treating amoebiasis & giardiasis. • Nosocomial infections can be prevented by: • Hand washing c. Using aseptic technique • Isolation of infected pts d. Proper use of antibiotics • Which organism is least detected in neonatal meningitis: • H. influenzaeb. S. aureus • Which organism is anaerobic: • Clostridium b. S. aureus c. Enterobacter • Which drug affects plasmids in micro-organisms: • Norfloxacin b. Cephalexin Treated with gentamycin Treated with silver nitrate
Which of the following bactericidal drugs cannot be given orally: • Streptomycin c. INH • PASA • Which of the following would be the best prophylaxis against TB: • INH c. Penicillin • Streptomycin • Mode of transmission of rabies (viral infections): • Saliva on an infected animal c. Direct contact • Inhalation of nasal secretions • Route of transmission of malaria (Plasmodium vivax, P. falciparum & P. malaria) is: • Mosquito bite b. Contact or droplet infection. • Which of the following agents is not an antifungal: • Tolnaftate. c. Metronidazol. • Miconazole. • Which of the following is considered to be an effect of the antibiotic on the host cell: • Affects the cell membrane b.Affects the cell wall • Affects folic acid metabolism c. None of the above • What damage is common to pathogen & host cell: • Cell membrane c.Cell wall • Cytoplasm • On which part of the penicillin molecule does the oxidase (or amidase) enzyme act: • The side chain b. The b-lactam ring. • On which part of the penicillin molecule does the penicillinase enzyme act: • The side chain b.The b-lactam ring. • Trichomonas vaginalis is similar to: • Flagellated protozoa c.H. vaginalis • G +ve bacteria d. G –ve bacteria • The micro-organism with techoic acid in its cell wall is: • S. aureusc.E. coli • Chlamydia • Which of the following drugs can pass the BBB (or meningococcal encephalitis is best treated by): confirm the answer ??? • Penicillin. d. Cephalosporins. g. Vancomycin. • Tetracycline. e. Sulphadiazine. • Streptomycin f. Chloramphenicol.
The drug used in prophylaxis of malaria is: • Quinacrine c. Quinine • Chloroquine • Why is mycoplasma resistant to penicillin: • It is a G –ve organism c. It is a penicillinase producer • It has no cell wall • What is the causative organism of scarlet fever: • S. pyogenes c. Rubella virus • S. aureus • Which antibiotic is penicillinase resistant but not acid resistant: • Methicillin c. Oxacillin • Ampicillin d. Nafcillin • Which antibiotic is acid resistant but not penicillinase resistant : • Methicillin c. Oxacillin • Ampicillin d. Nafcillin • Which antibiotic is both acid resistant & penicillinase resistant : • Dicloxacillin c. Oxacillin • Cloxacillin d. Nafcillin • Which organism causes mitral valve prolapse (endocarditis) & may cause infection during tooth extraction: • S. viridans (a-hemolytic strept.) treated with penicillin V • S. aureus • Which of the following is classified as a broad-spectrum antibiotic: • Ampicillin c. Streptomycin. • Cloxacillin d. Penicillin G. • The organism against which either penicillin V or erythromycin can be prescribed is: • S. aureusc.S. pyogenes. • E. coli d. H. influenzae. • Influenza virus is transmitted by: • Respiration b. Direct contact • The difference between human & bacterial cell is: • Presence of cell wall b.Presence of cytoplasmic membrane
Conjunctivitis may be: • Viral c. Bacterial • Fungal d. Allergic • Acne is treated by: • Penicillin c. Fucidic acid • Tetracyclin • Chicken pox lesions are treated by: • Calamine c. Oak bath • Diphenhydramine • Schistozoma mansoni (most common in Africa) causes: • Liver cirrhosis • Which type of organism causes athletes foot: • Fungal (Tinea pedis) c. Protozoal • Bacterial d. Yeast • Which agent is used to treat athelete’s foot: • Tolnaftate c. Metronidazole • Nystatin • Herpes I virus is transmitted by while Herpes II virus is transmitted by : • Respiration or lesions / direct contact • Which is synonymous to Herpes Zoster: • Schingles d. Herpes Simplex • Which is the causative organism of syphilis: • Triponema palladium • Botulism is due to: • Exotoxin b.Endotoxin • Which is true about UTI: • More common during pregnancy • Most commonly caused by E. coli • Which agent(s) is used to treat N. gonorrhea: • Penicillin G + Probenicid c. Tetracycline • Procaine penicillin • Mantoux test is similar to: • The old tuberculin test
Schistozomiasis is treated by: • Praziquental • Which of the following is (are) viral disease: • Polio c. Measeles • Rabies d. Influenza • Tape worm is treated by: • Niclosamide • Which of the following is an anthelmentic: • Pyrivenium pamoate c. Penicillin • Pyrantel pamoate d. Cephalosporins • Sulfamethoxazole & trimethoprim: • Have the same spectrum d. Taken with water • Have synergistic action e. Must be shaken before use • TMP is more potent with SMZ • Which type of organism causes shock syndrome: • S. aureus • Which agent is used for prophylaxis of meningitis: • Sulphonamides (sulfisoxazole) • In newborns, erythromycin is used to prevent blindness caused by: • Chlamydia • Nosocomial infections are caused by: • P. aeruginosa c. E. coli • S. aureus • Which organism causes granulomas: • M. tuberculosis • Bacteruria & pyuria are related to: • UTIs c.Nephritis • Renal failure d. Glomerulonephritis • Which of the following is (are) used as antifungal for scalp infections: • Miconazole c. Tar • Metronidazole • Which of the following is (are) true about trimethoprim: • Inhibits dihydrfolate reductase enzyme • Has a larger molecular size than folic acid • Has higher affinity for the receptors
Which of the following causes photo-sensitivity: • Penicillin c. Thyroxine • Sulfa d. Tertacycline • Which oral antibiotic is available as chewable tablets: • Amoxicillin • Metronidazole is effective in all except: • Amebiasis c. Giardiasis • Trichomoniasis d. Gonorrhea • Which of the following is not a predisposing factor to infection: • Congenital heart malformation • 1st stage syphilis is characterized by: • Chancre • Endocarditis is treated by: • Penicillin • Influenzae vaccine might cause allergy because: • It is a protein of a killed virus • Acyclovir is used in: • Herpes simplex b. HIV • Acyclovir is available as: • Tablets c. Topical • Syrup d. Injection • Probenicid …….. the action of penicillin: • Potentiates • Al / Mg hydroxides …….. the action of penicillin: • Inhibit • Herpes simplex: • Is schingeles disease c. Affects peripheral nervous system • Affects central nervous system • Pyogens are removed from water by: • Filtration b. Distillation • Meningitis in adults is caused by: • N. meningitidis • Which of the following does not cause genital infection: • Chlamydia
Which organism can cause eye infections in new borns leading to blindness: • N. gonorrheab. E. coli • Penicillins have different spectra of activity because: • Difference in the side chains • TB may lead to: • Liquefied necrosis c. Gaseous necrosis • Gangrenous necrosis • Syphilis is treated by: • Penicillin + Probenicid • In community acquired pneumoniae, all can be used except: • Penicillin V • Diaper rash is complicated by: • Candida albicans • Hepatitis B is transmitted by: • Blood b. Sex c. Food • Hepatitis A is transmitted by: • Blood b. Sex c. Food • In antibiotic treatment, which is more affected: • PABA b. Folic acid c. Follinic acid • Penicillin is short acting because: • It has high rate of tubular excretion • Scabies can be treated by: • Gamma benzene hexachloride b. Benzoyl benzoate ?? c. Lindone ??? • Aminoglycosides: • Cause nephro / oto toxicity c. Prophylaxis in intra-abdominal surgery • treat severe G –ve infections d. Specific agents for G +ve infections • Which makes inclusion bodies with penicillin: • Cu b. Pb c. Zn d. Hg • Which of the following agents has the highest ability to penetrate bacterial cell wall: DrugpKa Methicillin 1.5 Oxacillin 2.0 Penicillin 3.0 Doxacillin 5.0 • Doxacillin b. Methacillin
The drug of choice (DOC) for treating endocarditis due to methicillin resistant staph. is: • Vancomycin c. Cephazolin • Vancomycin + gentamycin • DOC in bronchitis is: • Amoxicillin or Septrin ??? b. Erythromycin (DOC) • DOC in Otitis Media: • Penicillins c. Erythromycin • Sulpha • DOC for anaerobic bacteria: • Penicillin (1st) b. Vancomycin (2nd) • DOC for H. influenzae: • Ampicillin or amoxicillin c. SMX • 2nd or 3rd generation cephalosporin • DOC for Streptococcus pyogens: • Penicillin c. Erythromycin • Cephalosporin • DOC for the treatment of Chlamydia: • Tetracycline (doxycyclin) b. Erythromycin • DOC for the treatment of Gonorrhea: • Cephalexin b. Cefuroxime • DOC for the treatment of peritonitis: • Clindamycin c. Lincomycin • Ciprofloxacin d. Metronidazole • DOC for the treatment of Mycoplasma pneumonia: • Tetracycline c. Erythromycin • Clindamycin • DOC for the treatment of a pregnant female with UTI: • Ampicillins c. Amoxicillin • Cephalexin