Download
1 / 1
10 likes | 216 Views
CL=THETA(1)+THETA(2)*(CLcr/4.26) THETA (1)=0.56; rse=19.6 THETA(2)= 0.32; rse=37.5. POPULATION PHARMACOKINETICS OF CEFTRIAXONE IN INTENSIVE CARE UNIT (ICU) ADULT PATIENTS C Le Guellec (1), N Simon (2), D.Garot (3), R. Respaud (1), P Lanotte (4), H. Blasco (1), PF Dequin (3).

E N D
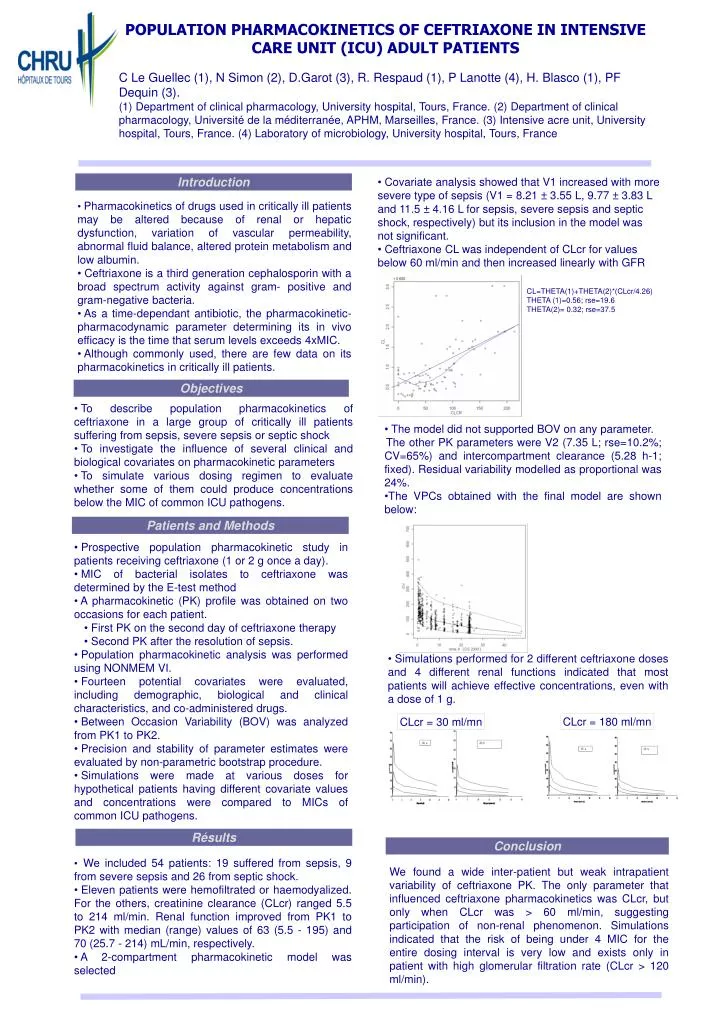
CL=THETA(1)+THETA(2)*(CLcr/4.26) THETA (1)=0.56; rse=19.6 THETA(2)= 0.32; rse=37.5 POPULATION PHARMACOKINETICS OF CEFTRIAXONE IN INTENSIVE CARE UNIT (ICU) ADULT PATIENTS C Le Guellec (1), N Simon (2), D.Garot (3), R. Respaud (1), P Lanotte (4), H. Blasco (1), PF Dequin (3). (1) Department of clinical pharmacology, University hospital, Tours, France. (2) Department of clinical pharmacology, Université de la méditerranée, APHM, Marseilles, France. (3) Intensive acre unit, University hospital, Tours, France. (4) Laboratory of microbiology, University hospital, Tours, France Introduction • Covariate analysis showed that V1 increased with more severe type of sepsis (V1 = 8.21 ± 3.55 L, 9.77 ± 3.83 L and 11.5 ± 4.16 L for sepsis, severe sepsis and septic shock, respectively) but its inclusion in the model was not significant. • Ceftriaxone CL was independent of CLcr for values below 60 ml/min and then increased linearly with GFR • Pharmacokinetics of drugs used in critically ill patients may be altered because of renal or hepatic dysfunction, variation of vascular permeability, abnormal fluid balance, altered protein metabolism and low albumin. • Ceftriaxone is a third generation cephalosporin with a broad spectrum activity against gram- positive and gram-negative bacteria. • As a time-dependant antibiotic, the pharmacokinetic-pharmacodynamic parameter determining its in vivo efficacy is the time that serum levels exceeds 4xMIC. • Although commonly used, there are few data on its pharmacokinetics in critically ill patients. Objectives • To describe population pharmacokinetics of ceftriaxone in a large group of critically ill patients suffering from sepsis, severe sepsis or septic shock • To investigate the influence of several clinical and biological covariates on pharmacokinetic parameters • To simulate various dosing regimen to evaluate whether some of them could produce concentrations below the MIC of common ICU pathogens. • The model did not supported BOV on any parameter. • The other PK parameters were V2 (7.35 L; rse=10.2%; CV=65%) and intercompartment clearance (5.28 h-1; fixed). Residual variability modelled as proportional was 24%. • The VPCs obtained with the final model are shown below: Patients and Methods • Prospective population pharmacokinetic study in patients receiving ceftriaxone (1 or 2 g once a day). • MIC of bacterial isolates to ceftriaxone was determined by the E-test method • A pharmacokinetic (PK) profile was obtained on two occasions for each patient. • First PK on the second day of ceftriaxone therapy • Second PK after the resolution of sepsis. • Population pharmacokinetic analysis was performed using NONMEM VI. • Fourteen potential covariates were evaluated, including demographic, biological and clinical characteristics, and co-administered drugs. • Between Occasion Variability (BOV) was analyzed from PK1 to PK2. • Precision and stability of parameter estimates were evaluated by non-parametric bootstrap procedure. • Simulations were made at various doses for hypothetical patients having different covariate values and concentrations were compared to MICs of common ICU pathogens. • Simulations performed for 2 different ceftriaxone doses and 4 different renal functions indicated that most patients will achieve effective concentrations, even with a dose of 1 g. CLcr = 180 ml/mn CLcr = 30 ml/mn Résults Conclusion • We included 54 patients: 19 suffered from sepsis, 9 from severe sepsis and 26 from septic shock. • Eleven patients were hemofiltrated or haemodyalized. For the others, creatinine clearance (CLcr) ranged 5.5 to 214 ml/min. Renal function improved from PK1 to PK2 with median (range) values of 63 (5.5 - 195) and 70 (25.7 - 214) mL/min, respectively. • A 2-compartment pharmacokinetic model was selected We found a wide inter-patient but weak intrapatient variability of ceftriaxone PK. The only parameter that influenced ceftriaxone pharmacokinetics was CLcr, but only when CLcr was > 60 ml/min, suggesting participation of non-renal phenomenon. Simulations indicated that the risk of being under 4 MIC for the entire dosing interval is very low and exists only in patient with high glomerular filtration rate (CLcr > 120 ml/min).