Download
1 / 18
190 likes | 450 Views
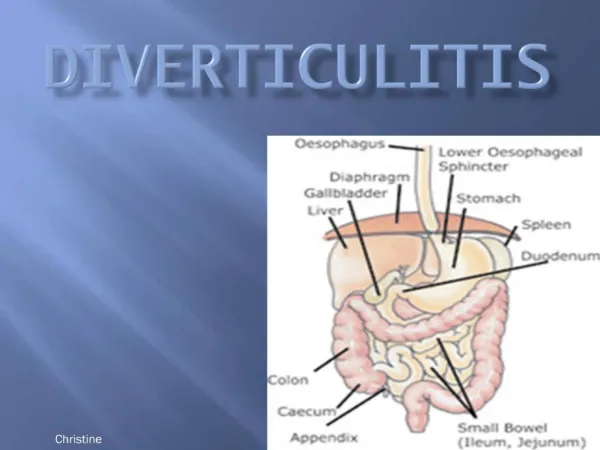
Diverticulitis. Identifying Data. R.T. 53 years old Male Filipino Employee High school graduate Roman Catholic Pasig City Reliability 80%. Chief Complaint. Left lower quadrant abdominal pain “ Pabalik-balik ang ‘ sakit ’ ng tiyan ko . ”. history. History.

E N D
Identifying Data • R.T. • 53 years old • Male • Filipino • Employee • High school graduate • Roman Catholic • Pasig City • Reliability 80%
Chief Complaint Left lower quadrant abdominal pain • “Pabalik-balikang ‘sakit’ ngtiyanko.”
History • Usual bowel movement: 2-3x daily, well-formed stools, after meals • Gradually developing abdominal pain, “kinakabag” colicky, LLQ, no precipitating signs or symptoms, starts prior to defecation, relieved with defecation, 7/10 • (-) fever, nausea, vomiting, hematuria, dysuria, acholic stools, hematochezia • Recurrent consults at company clinic/ E.R. • Meds: Motilium or Dysplatil • Temporarily relieved 2 years PTA
History • Sensation of recurrence of symptoms • Self-medicated Dysplatil TID w/ complete relief 1 year PTA
History 2 months PTA • Acute onset abdominal pain, colicky, LLQ, precipitated by inability to pass flatus, unrelieved with defecation, radiating to hypogastric area, 10/10, no specific timing, continuous • (+) nausea (-) fever, vomiting, hematuria, dysuria, acholic stools, hematochezia • CT scan: Diverticulitis • Meds for 2 weeks w/ complete relief • Ciprofloxacin 500mg/tab BID • Metronidazole 500mg/tab TID
History 1 month PTA • Recurrence of symptoms • (+) Tea-colored urine (-) fever, vomiting, dysuria, retention, trickling, flank pain • CT: suggests stone in ureter • Resumed medications w/ temporary relief • (+) Ciprofloxacin,Metronidazole 1week PTA • CT scan abdomen: no change in diagnoses • AP advised admission ADMISSION
Review of Systems • General. (+) Weight loss, weakness (-) Fever, fatigue • Musculoskeletal/ Dermatologic. (-) Rashes, change in skin color, lesions, joint swelling/ tenderness, gout • HEENT. (-) Dizziness, headache, blurring of vision, tinnitus, deafness, aural discharge, itchiness, earfulness, nosebleeds, frequent colds, hoarseness, enlarged LN • Respiratory. (-)Cough, dyspnea, hemoptysis, wheezing
Review of Systems • Cardiovascular. (-) Chest pain, palpitations, orthopnea, syncope • Gastrointestinal.(+) Poor appetite (-) Nausea, dysphagia, heartburn, change in bowel habits, rectal bleed, jaundice • Genitourinary. (-) Frequency, nocturia, dysuria, hematuria • Endocrine. (-) Excess sweat, polyuria, easy fatigability, easy bruisability, heat/cold intolerance • Extremities. (-) Edema
Past Medical History • GERD (1975) – Kremil-S • No history of asthma, allergies, HTN, DM, Pneumonia, Tuberculosis, Thyroid problems, or Trauma • Cannot recall immunization history
Family History • (+) Hypertension, Diabetes, Stroke, Lung cancer • No known history of Asthma, Allergies, Pneumonia, Tuberculosis, Kidney or Liver disease • No other family member presenting with the same symptoms or complaint
Personal and Social History • High school graduate • Machine operator, drug manufacturing • Non-smoker • Non-alcohol drinker • Denies illicit drug use/abuse • Diet: mainly on fish and vegetables • No regular exercise
Upon recent admission Physical examination
Physical Examination • General: Awake, alert, coherent, ambulatory, not in cardiorespiratory distress • Vital Signs:120/80, 81, 21, 36.6°C, Ht: 154cm, Wt: 52 kg, BMI: 21.5(normal range) • Skin: fair color, no rashes, lesions, no clubbing/pitting fingernails, • HEENT:anicteric sclera, pink palpebral conjunctiva, 2-3mm pupil BRTL, EOMs full and equal, non-sunken, no aural/otic discharge, no TPC, moist buccal mucosa, no CLAD, flat neck veins
Physical Examination • Respiratory: full, equal chest expansion, clear breath sounds, no rales/rhonchi/wheezes • Cardio: adynamicprecordium, apex 5th ICS LMCL, NRRR, distinct S1/S2, no murmurs • Abdomen: flat, soft, no lesions/ scars, hypoactive bowel sounds, no abdominal bruit, tympanic in all quadrants, direct tenderness 3-4/10 RUQ, no rebound, no guarding, no organomegaly (+) Rovsings, Obturator, Psoas(?) • Extremities: warm, full equal pulses, CRT <2secs, no edema