Download
1 / 43
470 likes | 1.13k Views
Practice Parameters for Sigmoid Diverticulitis. Janice F. Rafferty, M.D. Professor, University of Cincinnati Department of Surgery Chief, Division of Colon and Rectal Surgery Cincinnati, Ohio, USA. Practice Parameters for Sigmoid Diverticulitis. Paul Shellito , M.D.

E N D
Practice Parameters for SigmoidDiverticulitis Janice F. Rafferty, M.D. Professor, University of Cincinnati Department of Surgery Chief, Division of Colon and Rectal Surgery Cincinnati, Ohio, USA
Practice Parameters for SigmoidDiverticulitis Paul Shellito, M.D. Neil H. Hyman, M.D. W. Donald Buie, M.D. Standards Committee of The American Society of Colon and Rectal Surgeons Dis Colon Rectum 2006; 49: 939–944
Practice Parameters for SigmoidDiverticulitis Published literature from January 2000 to August 2005 was retrieved and reviewed. Searches of MEDLINE were performed by using keywords: diverticulitis, diverticulosis, peridiverticulitis, and fistula.
Levels of Evidence I Meta-analysis of multiple well-designed, controlled studies, randomized trials with low-false positive and low-false negative errors (high power) II At least one well-designed experimental study; randomized trials with high false-positive or high false-negative errors or both (low power) III Well-designed, quasi experimental studies, such as nonrandomized, controlled, single-group, preoperative-postoperative comparison, cohort, time, or matched case-control series IV Well-designed, nonexperimental studies, such as comparative and correlational descriptive and case studies V Case reports and clinical examples • Adapted from Cook DJ, Guyatt GH, Laupacis A, Sackett DL. Rules of evidence and clinical recommendations on theuse of antithrombotic agents. Chest 1992;102(4 Suppl):305S–11S
Grade of Recommendation A Evidence of type I or consistent findings from multiple studies of Type II, III, or IV B Evidence of Type II, III, or IV and generally consistent findings C Evidence of Type II, III, or IV but inconsistent findings D Little or no systematic empirical evidence
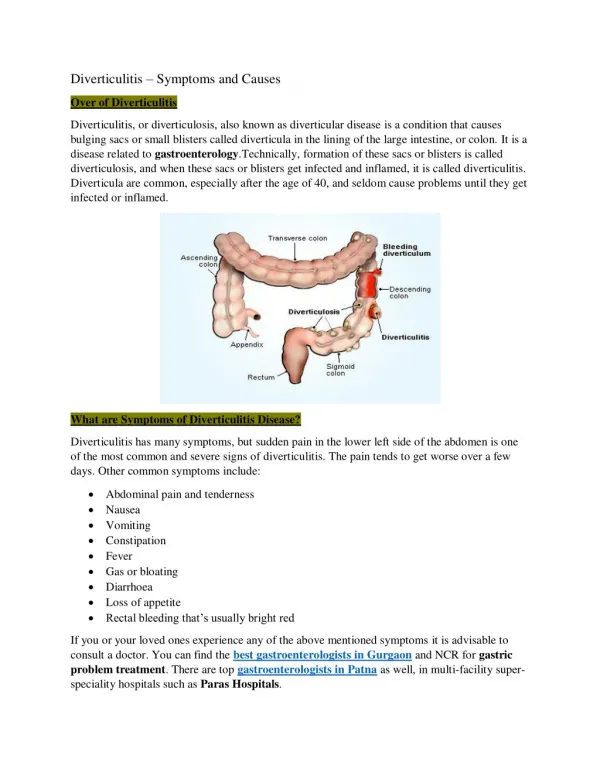
Statement of the Problem Acquired colonic diverticular disease affects the sigmoid colon in 95 percent of cases. Thirty-five percent of patients with sigmoid diverticulosis also have more proximal diverticuli Diverticula are rare below the pelvic peritoneal reflection. Prevalence correlates with age: * 30 percent by age 60 years * 60 percent of those 80 years and older 10-25 % of those with diverticulosis -> diverticulitis
Diverticular Disease • 2.2 million cases (2 billion dollars) Sandler Gastroenterology 2002 • Health care costs- $1.7 trillion www.cms.hhs.gov/statistics (accessed 4/1/2005)
Diverticular Disease-Etiology • Deficiency of dietary fiber (Burkitt and Painter Lancet 1972, Backo BJS 2001:88:1595, Aldoori AM J Clin Nutr 1994) • Segmentation and high intra-colonic pressures • Aging (decreased tensile strength of collagen and muscle fibers) • Hereditary disorders (Marfan’s and Ehler’sDanlos syndrome)
Initial Diagnosis History and physical exam Helpful tests: KUB, CBC, urinalysis (V,D) Alternative diagnoses: *irritable bowel syndrome * gastroenteritis * bowel obstruction * IBD * appendicitis *ischemic colitis * colorectal cancer *urinary tract infection *kidney stone *gynecologic disorder
Acute DiverticulitisMaking the Diagnosis Signs and Symptoms Fever Leukocytosis left lower quadrant pain with or without mass
Initial Diagnosis: CT Scan Accuracy enhanced by enteral contrast Highly sensitive and specific High PPV for inflammation and wall thickness Can identify complications “Severity staging” possible III, A
CT Scan: Severity Staging More severe inflammation predictive of * Failure of medical management * Future complications Detry R, James J, Kartheuser A, et al. Acute localizeddiverticulitis: optimum management requires accuratestaging. IntJ Colorectal Dis 1992;7:38–42 Chautems RC, Ambrosetti P, Ludwig A, MermillodB,MorelP, Soravia C. Long-term follow-up after firstacute episode of sigmoid diverticulitis: is surgery mandatory? A prospective study of 118 patients. DisColon Rectum 2002;45:962–6
Mild Localized sigmoid wall thickening (>5 mm) Inflammation of pericolic fat Severe Abscess Extraluminal air Extraluminal contrast Ambrosetti et al Dis Colon Rectum 2000:43:1363-7 CT Criteria to assess severity of Diverticulitis
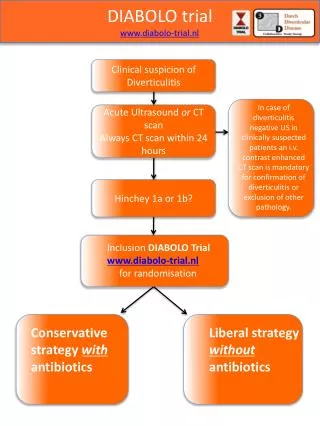
Acute Diverticulitis Hinchey Classification • Stage IPericolic Abscess • Stage II Pelvic, Retroperitoneal or intra-abdominal abscess • Stage III Purulent Peritonitis • Stage IV Fecal Peritonitis Hinchey et al Adv Surg 1978:12:85-105.
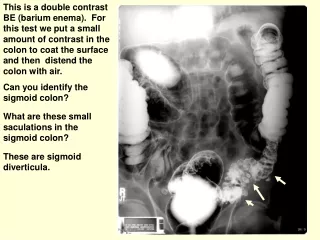
Diagnosis: Other modalities Ultrasound Barium enema Flexible sigmoidoscopy Cystoscopy III, B
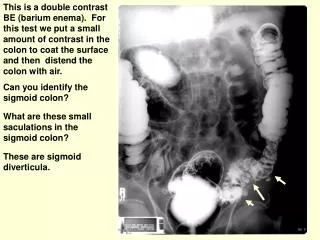
Acute Diverticulitis Contrast enema findings • “Deformed diverticula” • Extravasation of contrast • Intramural fistulization • Spasm • Stricture • Diverticulosis
Medical treatment of acute diverticulitis Nonoperative treatment typically includes dietary modification and oral or intravenous antibiotics (III, B) Successful in 70-100 % of patients. OUTPATIENT MANAGEMENT: appropriate IF NO * fever * excessive vomiting * marked peritonitis Must have opportunity for follow-up Patient should be able to take liquids and antibiotics PO
CT guided drainage 15% will have pelvic or mesenteric abscess >2cm abscess: in patient care plus drainage <2cm: may resolve without drainage May allow multi-staged approach Stoma avoidance III, B
Role of Percutaneous Drainage • Well Defined Abscess • “Radiologic Window” • Contraindicated in patients with generalized peritonitis or pneumoperitoneum • Generally NOT necessary for patients with small pericolicabscesses
Emergency surgery for acute diverticulitis (III, B) Severe or diffuse peritonitis (Hinchey 3,4) Failure of medical management Surgical options: * Hartman’s procedure * primary anastomosis (Hinchey 2-3) * anastomosis with proximal diversion
Elective surgery after uncomplicated diverticulitis Evaluate on case by case basis 1/3 will have episode within one year Additional 1/3 will have a third attack Elective resection may not decrease likelihood of complications Worst episode=first episode III, B
Elective surgery after uncomplicated diverticulitis CT graded severity predictive of natural history: more sever= worse outcome Inability to exclude carcinoma Immunosuppression
Natural history of diverticulitis Age/Severity on CT n Poor Outcome Probability at 5 yrs <50/Mild 14 6 36 <50/Severe 14 9 54% >50/Mild 74 16 19 >50/Severe 16 7 44% Chautems et al Dis Colon Rectum 2002;45:962-966
Diverticulitis and Renal Disease • 184 renal failure patients • 59 PKD • 125 ESRD • 12 pts with PKD had acute diverticulitis versus 4 of non-PKD (20% v. 3%) • 50% required surgery • Suggested diverticular disease may be an extrarenal manifestation of PKD Lederman AM Surg 2000;66:200-3
Young patients with diverticulitis Virulence appears to be no different Male predominance Longer life=increased cumulative risk? Younger patients more likely to present with severe disease
Diverticulitis in Young Patients • 40 patients - < 50 years old • 25% - surgery on first admission • Two- thirds did not require surgery during the follow-up period of 4-9 years Vignati et al Dis Colon Rectum 1995;38:627-629.
Diverticulitis in Young Patients:retrospecive review: 5,499 patients • 962 <50 years; 411 had CT with 1st episode of disease • 335 (81%) uncomplicated diverticultitis- 234 were followed nonoperatively. 28% recurrent uncomplicated episode, 4% recurrent complicated episode 2% required emergent operation and colostomy. • 76 (19%) complicated diverticultitis 23 emergent surgery, 38 elective surgery, 15 non-operative management • 7/15 recurrent uncomplicated episode • None required emergent operation or colostomy. Nelson RS, Velasco A, Mukesh BN. Dis Colon Rectum. 2006 Sep;49(9):1341-5
Young patients with diverticulitis < 40 years >40 years Severe 72% 35% p<.02 Emergent Op 40% 13% p<.04 *Pautrat K, Bretagnol F, Huten N, de Calan L. Department of Digestive Surgery, Trousseau Hospital, Tours, France. Dis Colon Rectum. 2007 Apr;50(4):472-7
Complicated diverticulitis Abscess Stricture Fistula Bleeding
Complicated diverticulitis 41% will develop severe recurrent sepsis Elective resection following abscess drainage recommended III, B Kaiser AM, Jiang JK, Lake JP, Atrinvan A, Gonzalez-Ruiz C, Beart RW Jr. Am J Gastroenterol. 2005 Apr;100(4):910-7
Non-operative management of Complicated diverticulitis Retrospective study- 256 patients with complicated diverticulitis on CT; 99 managed non-operatively Patient outcomes were reviewed. 46% had a recurrent episode 20 underwent a sigmoid colon resection, 1 required stoma No recurrence resulted in emergency resection Nelson RS, Ewing BM, Wengert TJ, Thorson AG. Am J Surg. 2008 Dec;196(6):969-72
Extent of resection Proximal margin: pliable colon without hypertrophy or inflammation Distal margin: splay of taenia Risk of recurrence higher with colosigmoid anastomosis III, B
Level of Anastomosis and Recurrent Diverticulitis Anastomosis Number Recurrence # (%) Colocolostomy 321 40(12.5) Coloproctostomy 180 12(6.7) Total 501 52 Benn et al Am J Surg 1986;151:269-71
Laparoscopy for diverticulitis Appropriate in selected patients No increase in complications Cost and outcomes comparable III, A
Conclusions • Timingand need for surgical treatment of sigmoid diverticular disease remains a topic of controversy. • Elective surgery for diverticulitis can be avoided in patients with uncomplicated disease, regardless of the number of recurrent episodes. • Ageof the patientshould not influence need for elective surgery • Clinical exam, and radiologic severity index, help determine which patients need operation
Thank you Janice Rafferty, MD University of Cincinnati Division of Colorectal Surgery 2123 Auburn Avenue Suite 524Cincinnati, Ohio 45219 (513) 929-0104