Download
1 / 27
460 likes | 1.5k Views
TRACHEA AND THORACIC DUCT. DR GARIMA SEHGAL. TRACHEA. Organization and Functions of the Respiratory System . Upper respiratory tract (nose to larynx) and Lower respiratory tract ( trachea onwards). The Trachea windpipe .

E N D
TRACHEA AND THORACIC DUCT DR GARIMA SEHGAL
Organization and Functions of the Respiratory System Upper respiratory tract (nose to larynx) and Lower respiratory tract ( trachea onwards).
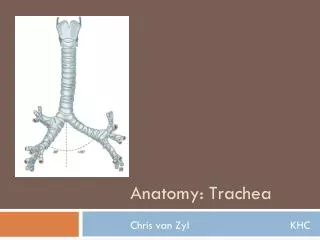
The Trachea windpipe • is a tubular passageway for air which extends as continuation of larynx • Is membrano-cartilaginous Measurements • Length - 12 cm • External diameter 2.5 cm • Internal diameter adults – 12mm newborn upto 3rd year- 3mm
Course – • Begins – lower border of cricoidcartilage/ C6 verterbra • Extends through the mediastinum and lies anterior to the esophagus • At the level of the sternal angle, the trachea bifurcates into two smaller tubes, called the right and left primary bronchi. • Each primary bronchus • projects laterally toward • each lung. • Level of Bifurcation • Cadaver -T4 • Living and standing -T6 • Newborn – T3
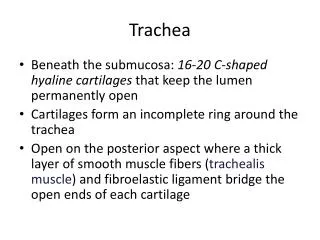
Structure • Anterior and lateral walls supported by 15 to 20 C-shaped tracheal cartilages. • Posterior part of tube lined by trachealis muscle What is the benefit of not having complete rings of tracheal cartilage between the trachea and the esophagus? The most inferior tracheal cartilage separates the primary bronchi at their origin and forms an internal ridge called the carina.
Microscopic anatomy Layers of the tracheal wall, from deep to superficial, are (1) the mucosa, (2) the submucosa, (3) media, or middle tunic, and (4) the adventitia.
Arterial supply mainly inferior thyroid arteries, bronchial arteries • Venous drainage mostly inferior thyroid veins • Lymphatic drainage pretracheal and paratracheal nodes • Nerve supply sensory, glands,trachealis parasympathetic (vagus) also sympathetic
Development the respiratory system begins as an outgrowth of the foregut just anterior to the pharynx. This outgrowth is called the respiratory diverticulum As the respiratory diverticulum elongates, its distal end enlarges to form a globular tracheal bud, which gives rise to the trachea. Soon after, the tracheal bud divides into bronchial buds, which branch repeatedly and develop with the bronchi.
TOF • The trachea goes to the lungs. • The esophagus and goes to the stomach. • They run side-by-side through the neck and upper chest. • During development a single tube divides to form the esophagus and the trachea. • sometimes the wall does not form properly and a tracheal esophageal fistula and/or esophagealatresia may be the result.
Lymphatic System • Consists of three parts • A network of lymphatic vessels (lymphatics) • Lymph • Lymph nodes
Lymphatic vessels begin as lymphatic capillaries. • Lymphatic capillaries are found throughout the body except in avascular tissues, the central nervous system, portions of the spleen, and red bone marrow. • Is lymph more similar to blood plasma or to interstitial fluid? Explain your answer.
Lymph vessels (lymphatics) include: • Lymphaticcapillaries • Lymphatic collecting vessels • Lymphatic trunks and ducts • If lymph flow blocked = tissue swelling or edema • Specialized lymphatic capillaries in vili of small intestine transport lipids - they are called lacteals, and the fluid is called chyle.
Lymphatic vessels join to form lymphatic trunks. • Lymphatic trunks join to form lymphatic ducts. 1)Thoracic duct 2)Right lymphatic duct • These empty into subclavian veins at junction with internal jugular vein.
Thoracic duct • Is an elongated common lymphatic trunk which conveys chyle and most of lymph of the body to the blood stream • Beaded in appearance • Has many valves • Length – 45 cm • Average width – 0.5 cm
Course Beginning – at upper end of cisternachyli at upper border of T12 • Enters thorax through aortic opening and traverses posterior mediastinum behind oesophagous • Opposite T5 inclines left, runs upwards Termination - at root of neck in the angle formed by junction of left subclavian and internal jugular vein
Relations • At aortic opening • At posterior mediastinum • In superior medistinum • At root of neck
Tributaries • Descending lymph trunks • Ascending lymph trunks • Left jugular lymph trunk • Left subclavian lymph trunk • Vessels draining upper six intercostal spaces
Drainage territory • Drains lymphatics from whole of the body • except -the right side of Head and neck, -Right upper limb, -Right lung and thoracic wall -right half of heart - convex surface of liver
Thoracic duct laceration • is vulnerable to damage after thoracic surgery and particularly after oesophageal surgery • The incidence is between 0.2 and 3% • Thoracic duct laceration is a potentially life-threatening complication: mortality rates are more than 50% with conservative management and as high as 10-16% even after early surgical duct ligation. • Rupture leads to leakage of chyle, which is rich in lipid, protein and lymphocytes and hence a progressive nutritional and immune deficit occurs • Chylous effusions due to damage to some of the tributaries of the thoracic duct, rather than to the duct itself are usually self-limiting and respond to conservative treatment
May be obstructed by mature filarial parasites producing bursting of lymph vessels. • Causes collection of chylous fluid in pleural and peritoneal sacs , chyloushydrocele etc.