Download
1 / 109
1.1k likes | 1.47k Views
Bursitis, Tendonitis, Fibromyalgia, and RSD. Joe Lex, MD, FAAEM Temple University School of Medicine Philadelphia, PA joe@joelex.net. Objectives. Explain how bursitis and tendonitis are similar Explain how bursitis and tendonitis differ from from another

E N D
Bursitis, Tendonitis, Fibromyalgia, and RSD Joe Lex, MD, FAAEM Temple University School of Medicine Philadelphia, PA joe@joelex.net
Objectives • Explain how bursitis and tendonitis are similar • Explain how bursitis and tendonitis differ from from another • List phases in development and healing of bursitis and tendonitis
Objectives • List common types of bursitis and tendonitis found at the: • Shoulder • Elbow • Wrist 5. List indications / contraindications for injection therapy of bursitis and tendonitis • Hip • Knee • Ankle
Objectives • Describe typical findings in a patient with fibromyalgia • Describe typical findings in a patient with reflex sympathetic dystrophy
Sports • Society more athletic • Physical activity health benefits • Overuse syndromes increase • 25% to 50% of participants will experience tendonitis or bursitis Intro
Workplace Musculoskeletal disorders from… …repetitive motions …localized contact stress …awkward positions …vibrations …forceful exertions • Ergonomic design incidence Intro
Bursae • Closed, round, flat sacs • Lined by synovium • May or may not communicate with synovial cavity • Occur at areas of friction between skin and underlying ligaments / bone Intro
Bursae • Permit lubricated movement over areas of potential impingement • Many are nameless • ~78 on each side of body • New bursae may form anywhere from frequent irritation Intro
Inflamed by… …chronic friction …trauma …crystal deposition …infection …systemic disease: rheumatoid arthritis, psoriatic arthritis, gout ankylosing spondylitis Bursitis Intro
Bursitis • Inflammation causes bursal synovial cells to thicken • Excess fluid accumulates inside and around affected bursae Intro
Tendons • Tendon sheaths composed of same synovial cells as bursae • Inflamed in similar manner • Tendonitis: inflammation of tendon only • Tenosynovitis: inflammation of tendon plus its sheath Intro
Tendons • Inflammatory changes involving sheath well documented • Inflammatory lesions of tendon alone not well documented • Distinction uncertain: terms tendonitis and tenosynovitis used interchangeably Intro
Tendons • Most overuse syndromes are NOT inflammatory • Biopsy: no inflammatory cells • High glutamate concentrations • NSAIDs / steroids: no advantage • TendonITIS a misnomer Intro
Bursitis / Tendonitis • Most common causes: mechanical overload and repetitive microtrauma • Most injuries multifactorial Intro
Bursitis / Tendonitis • Intrinsic factors: malalignment, poor muscle flexibility, muscle weakness or imbalance • Extrinsic factors: design of equipment or workplace and excessive duration, frequency, or intensity of activity Intro
Immediate Phase • Release of chemotactic and vasoactive chemical mediators • Vasodilation and cellular edema • PMNs perpetuate process • Lasts 48 hours to 2 weeks • Repetitive insults prolong inflammatory stage Phase
Healing Phase • Classic inflammatory signs: pain, warmth, erythema, swelling • Healing goes through proliferative and maturation • 6 to 12 weeks: organization and collagen cross-linking mature to preinjury strength Phase
History • Changes in sports activity, work activities, or workplace • Cause not always found • Pregnancy, quinolone therapy, connective tissue disorders, systemic illness History
History • Most common complaint: PAIN • Acute or chronic • Frequently more severe after periods of rest • May resolve quickly after initial movement only to become throbbing pain after exercise History
In joint capsule Joint pain / warmth / swelling Worse with active & passive movement All parts of joint involved Periarticular Pain not uniform across joint Pain only certain movements Pain character & radiation vary Articular vs. Periarticular
Physical Exam • Careful palpation • Range of motion • Heat, warmth, redness Exam
Lab Studies • Screening tests: CBC, CRP, ESR • Chronic rheumatic disease: mild anemia • Rheumatoid factor, antinuclear antibody, antistreptolysin O titers, and Lyme serologies for follow-up • Serum uric acid: not helpful Labs
Synovial Fluid • Especially crystalline, suppurative etiology • Appearance, cell count and diff, crystal analysis, Gram’s stain • Positive Gram’s: diagnostic • Negative Gram’s: cannot rule out Labs
Management • Rest • Pain relief: meds, heat, cold • No advantage to NSAIDs • Exceptions: olecranon bursitis and prepatellar bursitis have a moderate risk of being infected (Staphylococcus aureus) Rx
Management • Shoulder: immobilize few days • Risk of adhesive capsulitis • Lateral epicondylitis: forearm brace • Olecranon bursitis: compression dressing Rx
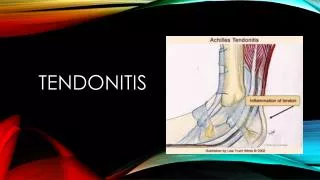
Management • De Quervain’s: splint wrist and thumb in 20o dorsiflexion • Achilles tendonitis: heel lift or splint in slight plantar flexion Rx
Local Injection • Lidocaine or steroid injection can overcome refractory pain • Steroids universally given, often with great success • No good prospective data to support or refute therapeutic benefit Rx
Local Injection • Short course of oral steroid may produce statistically similar results • Primary goal of steroid injection: relieve pain so patient can participate in physical rehab Rx
Local Injection • Adjunct to other modalities: pain control, PT, exercise, OT, relative rest, immobilization • Additional pain control: NSAIDs, acupuncture, ultrasound, ice, heat, electrical nerve stimulation Rx
Local Injection • Analgesics + exercise: better results than exercise alone • Eliminate provoking factors • Avoid repeat steroid injection unless good prior response • Wait at least 6 weeks between injections in same site Rx
Indications Diagnosis • Obtain fluid for analysis • Eliminate referred pain Therapy • Give pain relief • Deliver therapeutic agents Inject
Contraindication: Absolute • Bacteremia • Infectious arthritis • Periarticular cellulitis • Adjacent osteomyelitis • Significant bleeding disorder • Hypersensitivity to steroid • Osteochondral fracture Inject
Contraindication: Relative • Violation of skin integrity • Chronic local infection • Anticoagulant use • Poorly controlled diabetes • Internal joint derangement • Hemarthrosis • Preexisting tendon injury • Partial tendon rupture Inject
Preparations • Local anesthetic • Hydrocortisone / corticosteroid • Rapid anti-inflammatory effect • Categorized by solubility and relative potency • High solubility short duration • Absorbed, dispersed more rapidly Inject
Preparations • Triamcinolone hexacetonide: least soluble, longest duration • Potential for subcutaneous atrophy • Intra-articular injections only • Methylprednisolone acetate (Depo-Medrol®): reasonable first choice for most ED indications Inject
Dosage • Large bursa: subacromial, olecranon, trochanteric: 40 – 60 mg methylprednisolone • Medium or wrist, knee, heel ganglion: 10 – 20 mg • Tendon sheath: de Quervain, flexor tenosynovitis: 5 – 15 mg Inject
Site Preparation • Use careful aseptic technique • Mark landmarks with skin pencil, tincture of iodine, or thimerosal (Merthiolate®) (sterile Q-tip) • Clean point of entry: povidone-iodine (Betadine®) and alcohol • Do not need sterile drapes Inject
Technique • Make skin wheal: 1% lidocaine or 0.25% bupivacaine OR… …use topical vapocoolant: e.g., Fluori-Methane® • Use Z-tract technique: limits risk of soft tissue fistula • Agitate syringe prior to injection: steroid can precipitate or layer Inject
Complications: Acute • Reaction to anesthetic: rare • Treat as in standard textbooks • Accidental IV injection • Vagal reaction: have patient flat • Nerve injury: pain, paresthesias • Post injection flare: starts in hours, gone in days (~2%) Inject
Complications: Delayed • Localized subcutaneous or cutaneous atrophy at injection site • Small depression in skin with depigmentation, transparency, and occasional telangiectasia • Evident in 6 weeks to 3 months • Usually resolve within 6 months • Can be permanent Inject
Complications: Delayed • Tendon rupture: low risk (<1%) • Dose-related • Related to direct tendon injection? • Limit injections to no more than once every 3 to 4 months • Avoid major stress-bearing tendons: Achilles, patellar Inject
Complications: Delayed • Systemic absorption slower than with oral steroids • Can suppress hypopituitary-adrenal axis for 2 to 7 days • Can exacerbate hyperglycemia in diabetes • Abnormal uterine bleeding reported Inject
Bicipital Tendonitis • Risk: repeatedly flex elbow against resistance: weightlifter, swimmer • Tendon goes through bicipital (intertubercular) groove • Pain with elbow at 90° flexion, arm internally / externally rotated Shoulder
Bicipital Tendonitis • Range of motion: normal or restricted • Strength: normal • Tenderness: bicipital groove • Pain: elevate shoulder, reach hip pocket, pull a back zipper Shoulder
Bicipital Tendonitis • Lipman test: "rolling" bicipital tendon produces localized tenderness • Yergason test: pain along bicipital groove when patient attempts supination of forearm against resistance, holding elbow flexed at 90° against side of body Shoulder
Calcific TendonitisSupraspinatus Tendonitis Subacromial Bursitis • Calcific (calcareous) tendonitis: hydroxyapatite deposits in one or more rotator cuff tendons • Commonly supraspinatus • Sometimes rupture into adjacent subacromial bursa • Acute deltoid pain, tenderness Shoulder
Calcific TendonitisSupraspinatus TendonitisSubacromial Bursitis • Clinically similar: difficult to differentiate • Rotator cuff: teres minor, supraspinatus, infraspinatus, subscapularis • Insert as conjoined tendon into greater tuberosity of humerus Shoulder
Calcific TendonitisSupraspinatus TendonitisSubacromial Bursitis Jobe’s sign, AKA “empty can test” • Abduct arm to 90o in the scapular plane, then internally rotate arms to thumbs pointed downward • Place downward force on arms: weakness or pain if supraspinatus Shoulder