Download
1 / 61
640 likes | 1.04k Views
Acute Heart Failure Kendra Marsh, MD Clinical Instructor, Cardiology Fellow Department of Cardiology University of Illinois at Chicago. Objectives. Definitions Epidemiology Pathophysiology Diagnosis Management Summary of Guidelines Recommended Reading. Definitions Epidemiology

E N D
Acute Heart Failure Kendra Marsh, MD Clinical Instructor, Cardiology Fellow Department of Cardiology University of Illinois at Chicago
Objectives • Definitions • Epidemiology • Pathophysiology • Diagnosis • Management • Summary of Guidelines • Recommended Reading
Definitions Epidemiology Pathophysiology Diagnosis Management Summary of Guidelines Recommended Reading
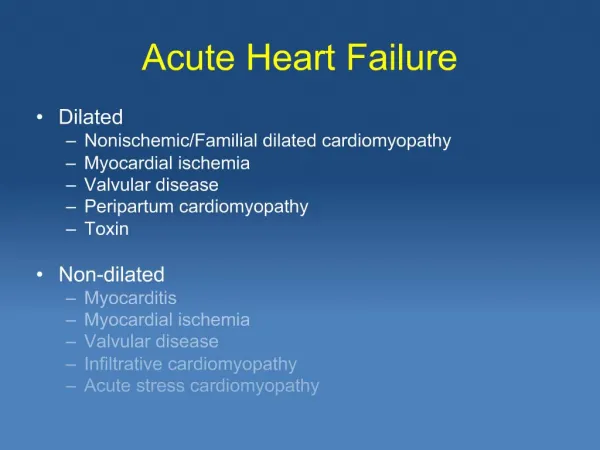
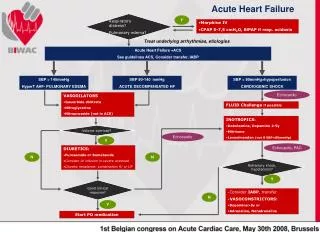
Acute Heart Failure • Rapid onset of symptoms and signs related to abnormal cardiac function • As a result of Systolic Dysfunction, Diastolic Dysfunction, Arrhythmias, or Preload-After load Mismatch
Related Clinical Conditions • De Novo or Chronic Decompensated • Hypertensive • Pulmonary Edema • Cardiogenic Shock • High Output Heart Failure: Arrhythmias, Thyrotoxicosis, Anemia, Paget’s Disease • Right Heart Failure
Stage I: No Heart Failure Stage II: Heart Failure S3 gallop, Pulmonary venous Hypertension, Rales <1/2 of the lung fields Stage III: Severe Heart Failure Frank pulmonary Edema, rales through out the lung field Stage IV: Cardiogenic Shock Systemic hypotension, peripheral vasoconstriction, endorgan failure, cyanosis, diaphoresis Killips Classification This classification system uses the clinical exam to determine the degree of cardiomyopathy after an acute MI.
Clinical Severity Classification Warm/Dry Warm/Wet Cold/Dry Cold/Wet • PERFUSION • CONGESTION • Auscultation of the lungs
Definitions Epidemiology Pathophysiology Diagnosis Management Summary of Guidelines Recommended Reading
Epidemiology • We have greatly improved our management of acute myocardial infarctions. • Large component of care is inpatient • Expensive to manage • High mortality in patients status post MI. • The leading cause of hospitalization in patients over 65 • 1 million hospitalizations per year with HF as primary diagnosis • 2.5 million hospitalizations with heart failure as secondary diagnosis
Definitions Epidemiology Pathophysiology Diagnosis Management Summary of Guidelines Recommended Reading
In an effort to maintain adequate tissue perfusion the body has three defenses: increase heart rate, vascular tone and circulating volume.
Definitions Epidemiology Pathophysiology Diagnosis Management Summary of Guidelines Recommended Reading
Definitions Epidemiology Pathophysiology Diagnosis Management Summary of Guidelines Recommended Reading
Oxygen • Class I, C • Improves oxygen delivery and tissue perfusion • Goal Saturation should be 95-98%, beyond that there is no indication for increased FIO2 • Always consider CPAP first or Non Invasive Positive Pressure Ventilation First • Endotrachial Intubation as a last resort
Pharmacotherapy • Morphine • Anticoagulation • Vasodilators • Diuretics • Beta Antagonists • Inotropic Agents
Morphine • Class IIb, B • Great Early in management • Venodilation • Mild Arterial Dilation • Slows Heart rate
Anticoagulation • No evidence to support anticoagulation for Acute Heart Failure alone • Yes in the case of Atrial Fibrillation • Yes in the case of LV thrombus • Large Placebo Control Trial with Enoxiparin at 40mg SC showed no mortality benefit
Nitrates: Class I, B Improves Cardiac Output and decreases PCWP Best with diuretics Low doses, venodilation High doses, arterial dilation Preload and Afteroad Good for 16-24 hours Sodium Nitroprusside: Class I, C Severe Heart Failure with Hypertension Primarily arterial dilation Need for arterial invasive monitoring Stop if active ischemia due to coronary steal phenomenon Vasodilators
Niseritide • Recombinant B-type Brain Naturetic Peptide • Venous, Arterial and coronary affects • Enhanced sodium excretion • Suppresses RAAS and sympathetic system
Vasodilators in the Management of Acute Heart Failure Trial (VAMC) • No good data to support adverse affects on renal function and niseritide • Retrospective analysis of VMAC showed potential for increased creatinin with increasing niseritide dose.
Diuretics • Class I, B
Diuretic Resistance can be associated with increased mortality.
RAPID-CHF Trial 40 patients ADHF and Renal Insufficiency (Cr >1.5) Ultrafiltration had significant increase in fluid removal after 24 hours 4650 L vs 2838L UNLOAD Trial 200 patients Renal insufficiency was not a criteria for inclusion Standard care vs ultra filtration 48 Hours 4.6 L vs 3.3L 90 Days fewer rehospitalizations .22 vs .46 and fewer unscheduled clinic visits 21 vs 44 Ultrafiltration Option in the setting of failed diuretic and vasodilator therapy
Beta Blockers • No data to support benefits in AHF • Traditionally considered a contra indication • Consider if there is active ischemia and blood pressure tolerates. • Ischemia and Tachycardia, Class IIb, C • Acute MI after stabilization, Class IIa, B • Chronic CHF after stabilization, Class I, A
Inotropic Agents • Peripheral Hypoperfusion refractory to vasodilators and diuretics, Class IIa, C • Danger: May increase oxygen demand and calcium loading
Dopamine: Vasodilator of Renal, Coronary, splanchnic and Cerebral Vascular beds Hypotensive patients Drawbacks: arrhythmia, increased pulmonary vascular resistance and increased afterload Dobutamine, Class IIa, C Hypotension and low Urine output Beta 1 and 2 agonist At high doses increases SVR Additive effect with Phosphodiesterase inhibitors Draw Backs- arrhythmia, reflex decrease in sympathetic tone Dopamine and Dobutamine
Phosphodiesterase Inhibitors • Milrinone and Enoximone • Hypoperfusion despite Diuretics and Vasodilators with good blood pressure. Class IIb, C • Lucitropic, Inotropic, vasodilator • Inhibits degredation of Cyclic AMP • Increase CO, CI, Stroke Volume, • Decrease PAP, PVR and PCWP • Immediate Action • Effect is Distal to Beta receptors, can be used in the setting Beta Blocker therapy. Class IIa, C
Outcomes of a Prospective Trial of Intravenous Milrinone For Exacerbations of Congestive Heart FailureOPTIME-CHF JAMA 2002
Levosimendan • Calcium ion sensitization • Also Pimobendon • Increases Contractility • A little PDI activity as well • Severe dysfunction with preserved blood pressure • Drawback: very pro-arrhythmogenic
LIDO Trial Levosimendan 24 hr infiusionvs Dobutamine 203 Patients Severe Decompensated HF, AHF, HF after CABG Excluded if cardiogenic shock Endpoints, increased CI (35% vs 25%) and reduced PCWP (28% vs 15%) in favor of Levosimendan SURVIVE Trial Levosimendan vs Dobutamine 24 hour therapy 1327 patients Endpoints symptomatic relief and BNP Levosimendan Greater reduction in BNP but no difference in symptomatic relief Clinical Trials
Pressors • Vasopressin: Cardiogenic shock in conjunction with inotropic therapy • Epinephrine B1 and B2, • Norepinephrine alpha receptors • Cardiac Glycosides: Inhibit cardiac Na/K ATPase, increases Ca/Na exchange mechanism. Tachycardia induced Cardiomyopathy.
Temporary Devices • IABP • Tandem Heart • ECMO • Ventricular Assist Devices
ECMO • ECMO removes carbon dioxide from and adds oxygen to venous blood via an artificial membrane lung Severe respiratory failure Cardiac Failure with inability to wean off Bypass Bridge to Cardiac Transplant
Temporary Devices:Tandem Heart pVAD • Continuous-flow centrifugal assist device placed extracorporeally • Cannula in femoral vein through intraatrial septum into LA • Pump withdraws oxygenated blood from the left atrium, propels it by a magnetically driven impeller through the outflow port • Blood returns into femoral artery via arterial cannula
Longer-term implantable devices • Novacor • HeartMate XVE • HeartMate II • Next Generation Devices