Download
1 / 29
290 likes | 442 Views
Proteinuria as a Surrogate Outcome in IgA Nephropathy. Ron Hogg MD Scott & White Medical Center Temple, Texas. Goals of Presentation. Overview of condition Observational studies Relationship between proteinuria and renal impairment in patients with IgA nephropathy

E N D
Proteinuria as a Surrogate Outcome in IgA Nephropathy Ron Hogg MD Scott & White Medical Center Temple, Texas
Goals of Presentation • Overview of condition • Observational studies • Relationship between proteinuria and renal impairment in patients with IgA nephropathy • Impact of various treatments (eg: ACEi, steroids, omega-3 fatty acids) on changes in proteinuria and progressive renal impairment • Relationship between early changes in proteinuria and subsequent fall in varying measures of GFR associated with these treatments
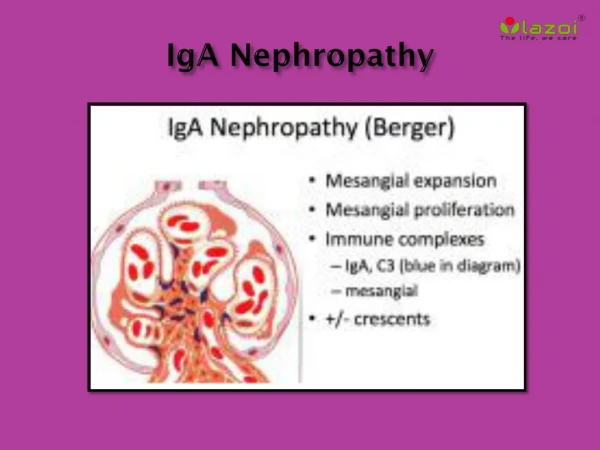
IgA Nephropathy: Background • Original description by Jean Berger in 1968 • Initially referred to as “Berger’s Disease” • Thought to have a benign outcome in ‘70s • Condition now known to be most common glomerular disease leading to ESRD worldwide
Definitions • Measures of Proteinuria • Collection: 24 hour urine excretion rates • Analyte: Total protein • Analytical methods: Variable • Early change: One year in most cases • Outcome measures • Measures of kidney disease progression • Kidney failure/ESRD • Decline in mGFR/eGFR • 50% increase in serum creatinine (Scr) • Mean slopes • mGFR/eGFR
IgA Nephropathy: Observational studies 1. Predicting Progression in IgA nephropathy. Bartosik et al. Am J Kidney Dis. 2001 2. Early prediction of IgAN progression: Proteinuria and AOPP are strong prognostic markers. Descamps-Latcha etal. Kidney Int. 2004
Predicting progression in IgANBartosik et al. AJKD: 2001 • Retrospective evaluation of the association between rate of decline of renal function (CG-GFR) and multiple variables in 298 adult patients with IgAN • Age at presentation: 36+/-13 years (16-73 years) • Follow-up from presentation: 70+/-46 months (range 12-231 months) • Age at biopsy: 37+/- 13 years (range 16-74 years) • Follow-up from renal biopsy: 57+/-44 months (range 12-227 months)
Bartosik et al. 2004Baseline clinical and laboratory data • CG-GFR: 76+/-35 ml/min (range 13-225 ml/min) • Serum creatinine: 1.54+/-1.0 mg/dl (0.5-8.4 mg/dl) • MAP-B: 102+/-15 mmHg (70-162mmHg) • UPEX-B: 2.3+/-2.3 g/day (0.1-21.6 g/day)
Bartosik et al.2004Variables monitored during follow-up • Slope of CG - GFR was derived from 10 +/- 7 values of serum creatinine in 90% of patients • Rate of decline of CG - GFR was -4.8 +/- 7.5 ml/min/year (0.4ml/min/month) • Five year renal survival rate from time of presentation was 80% • Ten year renal survival from presentation was 65%
Bartosik et al. 2004 Univariate analysis of factors associated with GFR decline
Bartosik et al. 2004Multiple Linear Regression Analysis • Using only clinical and laboratory data, the only independent predictors of slope were MAP-FU and UPEX-FU. The overall model was highly significant (p<0.001) • MAP and mean UPEX over progressively longer periods of follow-up were significantly associated with rate of deterioration of CG-GFR
Descamps-Latscha. KI: 2004 • Prospective cohort study of 120 adult patients identified between 1994 – 1997 and followed until the end of 2002 or start of dialysis • Primary end point defined as 50% reduction of CCr from baseline • Risk factors evaluated included CRP, UPEX and advanced oxidation protein products (AOPP) • 51 patients reached the end point, including 30 patients who had to start dialysis • Baseline UPEX was 0.59 +/- 0.62 g/day in 69 patients who did not reach the end point versus 2.67 +/- 1.28 mg/day in the 51 patients who did reach the end point
Descamps-Latscha. KI: 2004 1. Univariate Cox regression analysis showed age, proteinuria, hypertension, ACEi, CCr and AOPP levels to be significantly associated with renal outcome Proteinuria >1g/day HR (95% CI) = 16.41 (3.97-67.84, p=0.00001) 2. Multivariate analysis confirmed UPEX to be independent predictor of renal outcome a. With CCr included: HR = 7.78 (1.81-33.4, p=0.006) b. With CCr excluded: HR = 23.7 (5.35-104.8, p=0.0001) 3. Angiotensin II inhibitors were protective HR = 0.19 (0.09-0.44, p=0.001)
ACE inhibitors for IgA nephropathy • Treatment of IgA nephropathy with ACE inhibitors: A randomized contolled trial Praga et al. JASN: 2003
Praga et al: 2003 • RCT in 44 Patients with UPEX > 0.5g/day on 3 consecutive measurements and SCr <1.5mg/dl • Enrollment lasted 5 years (9/90-9/95) • 23 randomized to enalapril 5-40 mg/day • 21 randomized to control group • BP goal <140/90 mmHg in both groups • Follow-up: 78 months (E) vs 74 months (C) • Primary outcome: 50% increase in SCr
Praga et al: 2003 • Rx group: 3 pts (13%) reached end point • Controls: 12 pts (57%) reached end point, p<.05 • Renal survival at 4 years: 100% in Rx group, 70% in control group • Renal survival at 7 years: 92% in Rx group, 55% in control group, p<0.0 • Significant effect of the reduction in UPEX after 1 year of treatment was seen on renal survival Odds ratio=0.98, 95%CI 0.96-0.99, p=0.025
Omega-3 fatty acids in IgAN • Proteinuria patterns and their association with subsequent end stage renal disease in IgA nephropathy Donadio et al. Nephrol Dial Transplant: 2002
Donadio et al. 1992 • Examined data from 2 trials in patients with IgA nephropathy that had been conducted by the Mayo Collaborative Group to identify which determinants of proteinuria might provide the best predictors of ESRD after 1 year of treatment with O-3FA or placebo • UPEX was measured on 24 hour urines at baseline, 6 weeks, 6 months and 1 year in all patients
Donadio et al. 2002 There were 91 patients available for study after 1 year and 18 ESRD events after year one in Trial #1 There were 63 patients available for study after 1 year and 14 ESRD events after one year in Trial #2
Corticosteroids for IgA nephropathy 1. Steroid therapy during the early stage of progressive IgA nephropathy. A 10 year follow-up study Kobayashi et al. Nephron: 1996 2. Corticosteroids in IgA nephropathy: A randomized controlled trial. Pozzi et al. The Lancet: 1999 3. Steroid treatment for severe childhood IgA nephropathy:A randomized controlled trial. Yoshikawa et al. Clin J Am Soc Nephrol: 2006
Kobayashi et al. 1996 • Ten year + study of subset of patients (n=46) with UPEX 1-2 g/day, CCr >70ml/minute, severe renal histology • Original cohort of patients = 363 ( 90 with UPEX above). Previous report on these patients showed persistent UPEX > 1g/day to be associated with progressive renal impairment • Patients “allocated” to course of steroids or non-steroidal therapy, usually in order of renal bx • Steroids – 20 patients; “controls” – 26 patients
Pozzi et al. 1999 • RCT in 86 patients with IgAN who showed UPEX 1- 3.5g/day, plasma creatinine < 1.5g/day • Patients enrolled over 8 years (7/87-9/95) • Rx: Pulse IV MP 1g/day x 3 consecutive days on months 1, 3, 5 plus PO pred 0.5mg/kg/QOD x 6m • 43 patients randomized to the steroid group • 43 patients randomized to the control group who received supportive therapy (BP goal 140/90) • Study conducted in 7 renal units in Italy
Pozzi et al. 1999 • Risk of reaching the 50% increase in serum creatinine endpoint was 59% lower in steroid treated patients vs controls (relative risk 0.41, 95% CI 0.17-0.98, p=0.04) • When the reduction in UPEX from 0-6 months was added to the model, this covariate was selected as significant (RR 0.48, CI 0.34-0.69, p<0.0001), and the beneficial effect of steroid Rx was lost from the final model
Yoshikawa et al. 2006 • RCT conducted by the Japanese Pediatric IgA Nephropathy Treatment study Group • 83 children < 16 yrs of age enrolled in 20 centers - 50/83 pts ( 60%) detected by school screening • Rx group: pred, Imuran, warfarin, dipyridamole • “Control” group: prednisone. Rx duration 2 yrs • ACEi prohibited in both groups • Primary end point: disappearance of proteinuria • Secondary end point: percentage of sclerosed glomeruli on follow up renal biopsies
Conclusions • Severity of proteinuria is closely correlated with risk of progressive renal impairment in patients with IgA nephropathy • Reduction in proteinuria via multiple therapeutic interventions is associated with improvement in renal outcome • The impact of reducing proteinuria in this condition appears to be best attained when the lowering of proteinuria can be sustained