Download
1 / 1
10 likes | 267 Views
Comparison of Posteroanterior chest X-ray with thin slice HRCT for detection of pneumoconiosis Ann Murray 3 , Marek Mikulski 1 , Miriam B. Zimmerman 2 , Laurence Fuortes 1 1 Department of Occupational and Environmental Health, College of Public Health, The University of Iowa, Iowa City, IA

E N D
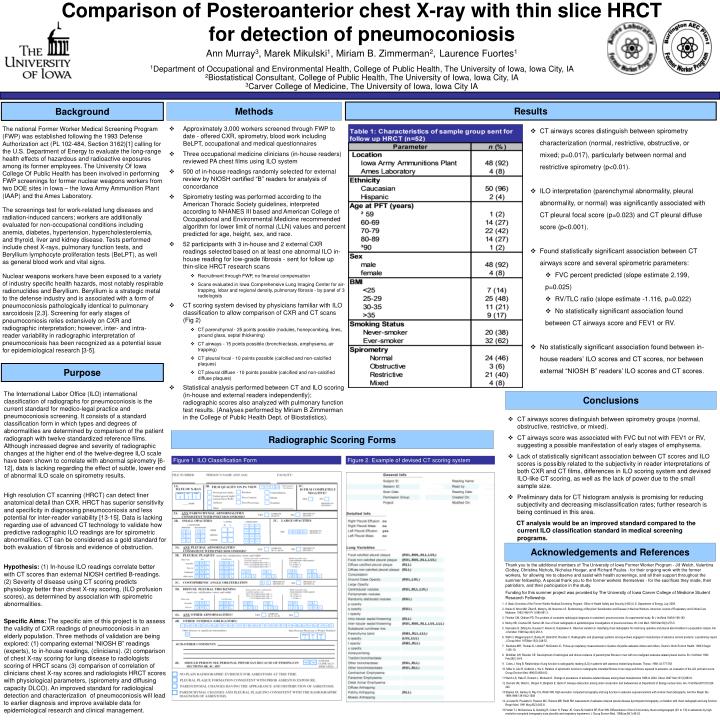
Comparison of Posteroanterior chest X-ray with thin slice HRCT for detection of pneumoconiosis Ann Murray3, Marek Mikulski1, Miriam B. Zimmerman2,Laurence Fuortes1 1Department of Occupational and Environmental Health, College of Public Health, TheUniversity of Iowa, Iowa City, IA 2Biostatistical Consultant, College of Public Health, TheUniversity of Iowa, Iowa City, IA 3Carver College of Medicine, The University of Iowa, Iowa City IA Results Methods Background • CT airways scores distinguish between spirometry characterization (normal, restrictive, obstructive, or mixed; p=0.017), particularly between normal and restrictive spirometry (p<0.01). • ILO interpretation (parenchymal abnormality, pleural abnormality, or normal) was significantly associated with CT pleural focal score (p=0.023) and CT pleural diffuse score (p<0.001). • Found statistically significant association between CT airways score and several spirometric parameters: • FVC percent predicted (slope estimate 2.199, p=0.025) • RV/TLC ratio (slope estimate -1.116, p=0.022) • No statistically significant association found between CT airways score and FEV1 or RV. • No statistically significant association found between in-house readers’ ILO scores and CT scores, nor between external “NIOSH B” readers’ ILO scores and CT scores. • Approximately 3,000 workers screened through FWP to date - offered CXR, spirometry, blood work including BeLPT, occupational and medical questionnaires • Three occupational medicine clinicians (in-house readers) reviewed PA chest films using ILO system • 500 of in-house readings randomly selected for external review by NIOSH certified “B” readers for analysis of concordance • Spirometry testing was performed according to the American Thoracic Society guidelines, interpreted according to NHANES III based and American College of Occupational and Environmental Medicine recommended algorithm for lower limit of normal (LLN) values and percent predicted for age, height, sex, and race. • 52 participants with 3 in-house and 2 external CXR readings selected based on at least one abnormal ILO in-house reading for low-grade fibrosis - sent for follow up thin-slice HRCT research scans • Recruitment through FWP, no financial compensation • Scans evaluated in Iowa Comprehensive Lung Imaging Center for air-trapping, lobar and regional density, pulmonary fibrosis - by panel of 3 radiologists • CT scoring system devised by physicians familiar with ILO classification to allow comparison of CXR and CT scans (Fig 2) • CT parenchymal - 25 points possible (nodules, honeycombing, lines, ground glass, septal thickening) • CT airways - 15 points possible (bronchiectasis, emphysema, air trapping) • CT pleural focal - 10 points possible (calcified and non-calcified plaques) • CT pleural diffuse - 10 points possible (calcified and non-calcified diffuse plaques) • Statistical analysis performed between CT and ILO scoring (in-house and external readers independently); radiographic scores also analyzed with pulmonary function test results. (Analyses performed by Miriam B Zimmerman in the College of Public Health Dept. of Biostatistics). The national Former Worker Medical Screening Program (FWP) was established following the 1993 Defense Authorization act (PL 102-484, Section 3162)[1] calling for the U.S. Department of Energy to evaluate the long-range health effects of hazardous and radioactive exposures among its former employees. The University Of Iowa College Of Public Health has been involved in performing FWP screenings for former nuclear weapons workers from two DOE sites in Iowa – the Iowa Army Ammunition Plant (IAAP) and the Ames Laboratory. The screenings test for work-related lung diseases and radiation-induced cancers; workers are additionally evaluated for non-occupational conditions including anemia, diabetes, hypertension, hypercholesterolemia, and thyroid, liver and kidney disease. Tests performed include chest X-rays, pulmonary function tests, and Beryllium lymphocyte proliferation tests (BeLPT), as well as general blood work and vital signs. Nuclear weapons workers have been exposed to a variety of industry specific health hazards, most notably respirable radionuclides and Beryllium. Beryllium is a strategic metal to the defense industry and is associated with a form of pneumoconiosis pathologically identical to pulmonary sarcoidosis [2,3]. Screening for early stages of pneumoconiosis relies extensively on CXR and radiographic interpretation; however, inter- and intra- reader variability in radiographic interpretation of pneumoconiosis has been recognized as a potential issue for epidemiological research [3-5]. Purpose The International Labor Office (ILO) international classification of radiographs for pneumoconiosis is the current standard for medico-legal practice and pneumoconiosis screening. It consists of a standard classification form in which types and degrees of abnormalities are determined by comparison of the patient radiograph with twelve standardized reference films. Although increased degree and severity of radiographic changes at the higher end of the twelve-degree ILO scale have been shown to correlate with abnormal spirometry [6-12], data is lacking regarding the effect of subtle, lower end of abnormal ILO scale on spirometry results. High resolution CT scanning (HRCT) can detect finer anatomical detail than CXR. HRCT has superior sensitivity and specificity in diagnosing pneumoconiosis and less potential for inter-reader variability [13-15]. Data is lacking regarding use of advanced CT technology to validate how predictive radiographic ILO readings are for spirometric abnormalities. CT can be considered as a gold standard for both evaluation of fibrosis and evidence of obstruction. Hypothesis: (1)In-house ILO readings correlate better with CT scores than external NIOSH certified B-readings. (2) Severity of disease using CT scoring predicts physiology better than chest X-ray scoring, (ILO profusion scores), as determined by association with spirometric abnormalities. Specific Aims: The specific aim of this project is to assess the validity of CXR readings of pneumoconiosis in an elderly population. Three methods of validation are being explored: (1) comparing external “NIOSH B” readings (experts), to in-house readings, (clinicians). (2) comparison of chest X-ray scoring for lung disease to radiologists scoring of HRCT scans (3) comparison of correlation of clinicians chest X-ray scores and radiologists HRCT scores with physiological parameters, (spirometry and diffusing capacity DLCO). An improved standard for radiological detection and characterization of pneumoconiosis will lead to earlier diagnosis and improve available data for epidemiological research and clinical management. Conclusions • CT airways scores distinguish between spirometry groups (normal, obstructive, restrictive, or mixed). • CT airways score was associated with FVC but not with FEV1 or RV, suggesting a possible manifestation of early stages of emphysema. • Lack of statistically significant association between CT scores and ILO scores is possibly related to the subjectivity in reader interpretations of both CXR and CT films, differences in ILO scoring system and devised ILO-like CT scoring, as well as the lack of power due to the small sample size. • Preliminary data for CT histogram analysis is promising for reducing subjectivity and decreasing misclassification rates; further research is being continued in this area. CT analysis would be an improved standard compared to the current ILO classification standard in medical screening programs. Radiographic Scoring Forms Figure 1. ILO Classification Form Figure 2. Example of devised CT scoring system Acknowledgements and References Thank you to the additional members of The University of Iowa Former Worker Program - Jill Welch, Valentina Clottey, Christina Nichols, Nicholas Hoeger, and Richard Paulos - for their ongoing work with the former workers, for allowing me to observe and assist with health screenings, and all their support throughout the summer fellowship. A special thank you to the former workers themselves - for the sacrifices they made, their patriotism, and their participation in the study. Funding for this summer project was provided by The University of Iowa Carver College of Medicine Student Research Fellowship. A Basic Overview of the Former Worker Medical Screening Program. Office of Health Safety and Security (HSS) U.S. Department of Energy, July 2009. Kreiss K, Mroz MM, Zhen B, Martyny JW, Newman LS. Epidemiology of Beryllium Sensitization and Disease in Nuclear Workers. American Journal of Respiratory and Critical Care Medicine. 1993;148(4 Pt 1):985-991.3. Fletcher CM, Oldham PD. The problem of consistent radiological diagnosis in coalminers’ pneumoconiosis. An experimental study. Br J Ind Med 1949;6:168-183. Mulloy KB, Coultas DB, Samet JM. Use of chest radiographs in epidemiological investigations of pneumoconioses. Br J Ind Med. 1993 Mar:50(3):273-5. Impivaara O, Zitting AJ, Kuusela T, Alanen E, Karjalainen A. Observer variation in classifying chest radiographs for small lung opacities and pleural abnormalities in a population sample. Am J Ind Med. 1998 Sep;34(3):261-5. Weill H, Waggenspack C, Bailey W, Ziskind M, Rossiter C. Radiographic and physiologic patterns among workers engaged in manufacture of asbestos cement products: a preliminary report. J Occup Med. 1973Mar;15(3):248-52. Becklake MR, Thomas D, Liddell F, McDonald JC. Follow-up respiratory measurements in Quebec chrysotile asbestos miners and millers. Scand J Work Environ Health. 1982;8 Suppl 1:105-10. McMillan GH, Rossiter CE. Development of radiological and clinical evidence of parenchymal fibrosis in men with non-malignant asbestos-related pleural lesions. Br J Ind Med. 1982 Feb;39(1):54-9. Cotes J, King B. Relationship of lung function to radiographic reading (ILO) in patients with asbestos related lung disease, Thorax. 1988; 43:777-783 Miller A, Lilis R, Godbold J, Wu X. Relation of spirometric function to radiographic interstitial fibrosis in two large workforces exposed to asbestos: an evaluation of the ILO profusion score. Occup Environ Med.1996;53:808-812 Welch LS, Haile E, Dement J, Michaels D. Change in prevalence of asbestos-related disease among sheet metalworkers 1986 to 2004. Chest. 2007 Mar;131(3):863-9. Dement JM, Welch L, Ringen K, Bingham E, Quinn P. Airways obstruction among older construction and tradeworkers at Department of Energy nuclear sites. Am J Ind Med.2010;53:224-240 Staples CA, Gamsu G, Ray CS, Webb WR. High resolution computed tomography and lung function in asbestos exposed workers with normal chest radiographs. Am Rev Respir Dis. 1989;1989:139:1502-1508 al Jarad N, Poulakis N, Pearson MC, Rubens MB, Rudd RM. Assessment of asbestos-induced pleural disease bycomputed tomography--correlation with chest radiograph and lung function. Respir Med. 1991 May;85(3):203-8. Harkin TJ, McGuinness G, Goldring R, Cohen H, Parker JE, Crane M, Naidich DP, Rom WN. Differentiation of the ILO boundary chest roentgenograph (0/1 to 1/0) in asbestosis by high-resolution computed tomography scan,alveolitis and respiratory impairment. J Occup Environ Med. 1996Jan;38(1):46-52. A B