Download
1 / 44
610 likes | 1.87k Views
Polycythemia Vera. Week 5 Case 3. Group B Ramos, Ronald Rangel, Erika Raymundo , Nikko Rayos , Karen Recio , Maria Kristina Reyes, Carmen Reyes, Jenilene Reyes, Lourdes. Rivera, Laila Rivere , Djeaune Robosa,Dean Rodas , Francis Rodriguez, Shereen Rogelio, Ma.Graciela

E N D
Polycythemia Vera Week 5 Case 3 Group B • Ramos, Ronald • Rangel, Erika • Raymundo, Nikko • Rayos, Karen • Recio, Maria Kristina • Reyes, Carmen • Reyes, Jenilene • Reyes, Lourdes • Rivera, Laila • Rivere, Djeaune • Robosa,Dean • Rodas, Francis • Rodriguez, Shereen • Rogelio, Ma.Graciela • Roque, Marianne
RP, 62 y.o. male • CC: Left sided body weakness
Review of Systems • Weight loss of 25% in the past 3 mos. • Have pruritus after showering • Occasional claudication
Past Medical History • Known Hypertensive (2yrs) • Maintained on amlodipine 5mg/tab od taken regularly • Non diabetic • No previous hospitalizations
Personal Social History • Non smoker • Occasional alcoholic drinker Family History • Unremarkable
Physical Exam • Conscious, coherent, ambulates with assistance, not in cardiorespiratory distress BP 130/90 CR 10bpm RR 21 cpm T 37.1C • Warm moist skin, plethora noted • Pink palpebral conjunctivae, anicteric sclera • Symmetrical chest expansion, no retrations, clear breath sounds • Adynamicprecordium, AB 5th LICS MCL • Flabby abdomen, normoactive bowel sounds, no hepatomegaly, obliterated Traube’s space • Extremities: no cyanosis, no edema, full and equal pulses
Physical Exam • Neuro Exam: • (+) slurring of speech • (+) shallow Left nasolabial fold • (+) tongue deviated to the right upon protrusion • MMT grade 2/5 on both left upper and lower extremitites • (-) Babinski
Laboratory Interpretation: Hemoconcentration, leukocytosis with thrombocytosis
Salient Features Pertinent Positives • Weight loss of 25% in the past 3 mos. • Have pruritus after showering • Occasional claudication • Hypertensive (BP 130/90) • Plethora • obliterated Traube’s space (splenomegaly) • Neuro Exam:(+) slurring of speech; (+) shallow Left nasolabial fold; (+) tongue deviated to the right upon protrusion; MMT grade 2/5 on both left upper and lower extremitites • Hemoconcentration, leukocytosis with thrombocytosis Pertinent Negatives • Extremities: no cyanosis, no edema, full and equal pulses • no hepatomegaly
Etiology • Exact etiology is unknown • Abnormalities in chromosome such as 20q, trisomy 8, and 9p, have been documented in up to 30% of untreated PV patients • A mutation in the autoinhibitory, pseudokinase domain of the tyrosine kinase JAK2 appears to have a central role in the pathogenesis of PV. • tyrosine kinase JAK2 replaces valine with phenylalanine (V617F), causing constitutive activation of the kinase
Clinical Features • Splenomegaly • High Hgb and Hct • Uncontrolled erythrocytosis • Hypervicosityleading to neurologic symptoms: vertigo, tinnitus, headache, visual disturbances, and TIAs. • Systolic hypertension • In some patients, venous or arterial thrombosis
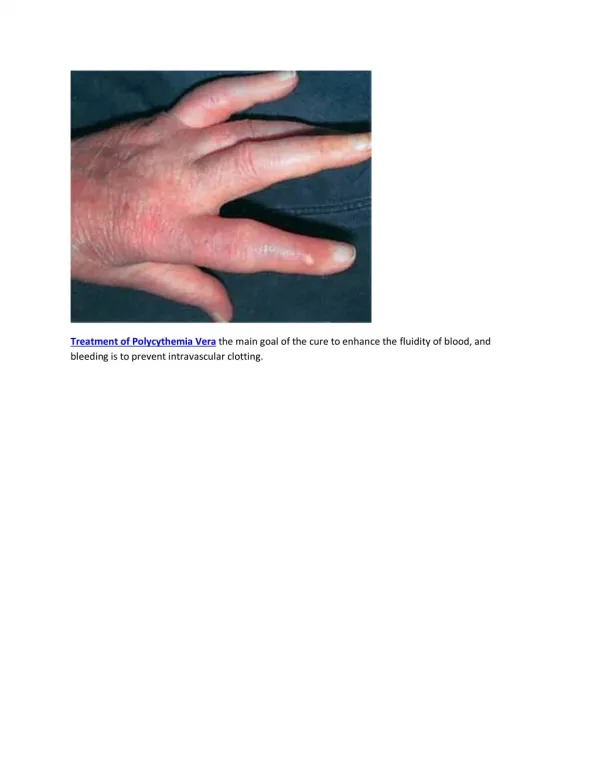
Clinical Features • Cerebral, cardiac, or mesenteric vessels are commonly involved • Intraabdominal venous thrombosis • Digital ischemia, easy bruising, epistaxis, acid-peptic disease, or gastrointestinal hemorrhage • Due to vascular stasis or thrombocytosis • Erythromelalgia • Erythema, burning and pain in extremities
Diagnosis • Presents with erythrocytosis in combination with leukocytosis, thrombocytosisor both • If Px presents with with an elevated hemoglobin or hematocrit alone, or with thrombocytosis alone, evaluation becomes more complex because of the many diagnostic possibilities • Unless hemoglobin is >20 gm% (hematocrit >60%), it is not possible to distinguish PV from disorders causing plasma volume contraction • Red cell mass and plasma volume determination mandatory to establish presence of absolute erythrocytosis Fauci et.al. Harrison’s principles of Internal Medicine 2008 17th edition. McGraw-Hill USA
Diagnosis • Once absolute erythrocytosis has been establisehd, its cause must be determined • An elevated plasma erythropoeitin level suggests either a hypoxic cause or autonomous production • Pulmonary function • Abdominal CT scan to evaluate renal and hepatic anatomy • Other labs: • RBC count • Mean corpuscular volume • Red cell distribution width ** bone marrow aspirate and biopsy provide no specific diagnostic information unless there is need to establish a myelofibrosis or exclude some other disorder Fauci et.al. Harrison’s principles of Internal Medicine 2008 17th edition. McGraw-Hill USA
Apparent / Relative Polycythemia True / Absolute Polycythemia Either a clonalmyeloproliferativedisorder (polycythemiavera) or a nonclonal increase in red blood cell mass that is often mediated by erythropoietin (secondary polycythemia) Either a decrease in plasma volume (relative polycythemia) or a misperception of what constitutes the upper limit of normal values for either hemoglobin or hematocrit Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
APPARENT POLYCYTHEMIA • Relative polycythemia • Conditions that cause acute depletion of plasma volume e.g. severe dehydration • The existence of chronic contraction of the plasma volume, such as postulated for: • Gaisböck'ssyndrome – relative polycythemia associated with hypertension and nephropathy • Stress / spurious polycythemia – relative polycythemia associated with emotional stress Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
ABSOLUTE / TRUE POLYCYTHEMIA • Polycythemiavera • Secondary polycythemia • Congenital • Associated with high or normal serum erythropoietin level • Associated with low serum erythropoietin level • Acquired • Erythropoietin mediated • Hypoxia-driven • Hypoxia-independent (pathologic erythropoietin production) • Drug associated • Unknown mechanism Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
Secondary Polycythemia • Congenital • Associated with high or normal serum erythropoietin level • Associated with low serum erythropoietin level • Acquired • Erythropoietin mediated • Hypoxia-driven • Hypoxia-independent (pathologic erythropoietin production) • Drug associated • Unknown mechanism Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
Secondary Polycythemia • Congenital • Associated with high or normal serum erythropoietin level • Associated with low serum erythropoietin level • Acquired • Erythropoietin mediated • Hypoxia-driven • Hypoxia-independent (pathologic erythropoietin production) • Drug associated • Unknown mechanism Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
Secondary Polycythemia: Congenital Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
Secondary Polycythemia • Congenital • Associated with high or normal serum erythropoietin level • Associated with low serum erythropoietin level • Acquired • Erythropoietin mediated • Hypoxia-driven • Hypoxia-independent (pathologic erythropoietin production) • Drug associated • Unknown mechanism Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
Secondary Polycythemia: Acquired Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
Secondary Polycythemia • Congenital • Associated with high or normal serum erythropoietin level • Associated with low serum erythropoietin level • Acquired • Erythropoietin mediated • Hypoxia-driven • Hypoxia-independent (pathologic erythropoietin production) • Drug associated • Unknown mechanism Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
Secondary Polycythemia: Acquired Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
Secondary Polycythemia • Congenital • Acquired • Erythropoietin mediated • Hypoxia-driven • Hypoxia-independent (pathologic erythropoietin production) • Drug associated • Erythropoietin doping • Treatment with androgen preparations • Unknown mechanism Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
Secondary Polycythemia • Congenital • Acquired • Erythropoietin mediated • Hypoxia-driven • Hypoxia-independent (pathologic erythropoietin production) • Drug associated • Unknown mechanism • Post–renal transplant erythrocytosis Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. Goldman: Cecil Medicine, 23rd ed.
Major clinical complications relate: • directly to increase in blood viscosity with red cell mass elevation AND • indirectly to increased turnover of red cells, leukocytes and and platelets with the attendant increase in uric acid and cytokine production • Cytokines appears to be responsible for the increase in peptic ulcer disease and for the pruritus associated with this disorder Harrison’s Principle of Internal Medicine 17th ed.
Sudden massive increase in spleen size can be associated with splenic infarction and progressive cachexia • Myelofibrosis appears to be part of the natural history of the disease but is a reactive, reversible process that does not itself impede hematopoiesis; in some patients, however, it is accompanied by significant extramedullaryhematopoiesis, hepatosplenomegaly, and transfusion dependent anemia Harrison’s Principle of Internal Medicine 17th ed.
Organomegalycan cause significant mechanical discomfort, portal hypertension, and cachexia • Erythromelalgia is a syndrome of unknown etiology associated with thrombocytosis, primarily involving the lower extremities and manifested usually by erythema, warmth, and pain of the affected appendage, and occasionally digital infarction - usually responsive to salicylates Harrison’s Principle of Internal Medicine 17th ed.
If left uncontrolled, erythrocytosis can lead to thrombosis involving vital organs such as the liver, heart, brain, or lungs • Patients with massive splenomegaly are particularly prone to thrombotic events because the associated increase in plasma volume masks the true extent of the red cell mass elevation as measured by the hematocrit of hemoglobin level Harrison’s Principle of Internal Medicine 17th ed.
Phlebotomy • Phlebotomy or bloodletting has been the mainstay of therapy • Remove excess cellular elements to improve the circulation of blood by lowering the blood viscosity • mainly red blood cells Harrison’s Principle of Internal Medicine 17thed http://emedicine.medscape.com/article/205114-treatment Jan 23, 2009
Phlebotomy • Patients with hematocrit values of less than 70% may be bled twice a week to reduce the hematocrit to the range of less than 45% • Patients with severe plethora who have altered mentation or associated vascular compromise can be bled more vigorously, with daily removal of 500 mL of whole blood Harrison’s Principle of Internal Medicine 17thed http://emedicine.medscape.com/article/205114-treatment Jan 23, 2009
Post-Phlebotomy • volume replacement with saline solution after each procedure to avoid postural hypotension • use myelosuppressive agents (Hydroxyurea) to avoid thrombotic or hemorrhagiccomplications http://emedicine.medscape.com/article/205114-treatment Jan 23, 2009
Hydroxyurea • effective agent for myelosuppression • Reduced the risk of thrombosis compared with phlebotomy alone and should be the drug of choice for patients older than 40 years • however, concerns have been raised regarding long-term risks for leukemic transformation Harrison’s Principle of Internal Medicine 17thed http://emedicine.medscape.com/article/205114-treatment Jan 23, 2009
Anagrelide (Agrylin) • A cyclic adenosine monophosphate phosphodiesterase inhibitor that prevents platelet aggregation and inhibits megakaryocyte maturation, thereby decreasing platelet counts • To date, this agent does not appear to increase the risk of acute leukemia in patients with PV and ET over time http://emedicine.medscape.com/article/205114-treatment Jan 23, 2009
References • Fauci, et al: Harrison’s Principles of Internal Medicine, 17th ed. • Goldman: Cecil Medicine, 23rd ed.