Download
1 / 41
460 likes | 1.35k Views
Post MI Ventricular Septal Defects. Nick Tehrani, MD. Overview. VSD Complicates 1-2% of cases of acute myocardial infarction. First successful correction reported by Cooley in 1957. Overview. High mortality despite various improvements in therapy 30 day mortality- 74% 1 year mortality- 78%

E N D
Post MI Ventricular Septal Defects Nick Tehrani, MD
Overview • VSD Complicates 1-2% of cases of acute myocardial infarction. • First successful correction reported by Cooley in 1957.
Overview • High mortality despite various improvements in therapy • 30 day mortality- 74% • 1 year mortality- 78% GUSTO analysis, Crenshaw et al, Circ. 1/2000
Overview • Relative Improvement in survival due to • Earlier diagnosis • Earlier flow restoration • More aggressive surgical intervention
Overview • Incidence declining due to: • Earlier restoration of flow, preventing transmural MI • More aggressive BP control post MI
Overview • Predictors of VSD • Advanced age, • Anterior location of infarction, • Female sex, • No history of smoking Per GUSTO analysis • Thrombolysis after 12 hours also suggested as a predisposing factor.
Overview • Average time to rupture • 2-4 days • Range: few hours 2 weeks • Time course may be accelerated by thrombolysis, possible related to intramyocardial hemorrhage
Overview • Coronary anatomy and VSD • Post MI VSDs more commonly associated with 100% occlusion of the infarct related artery • This was observed in all of our patients
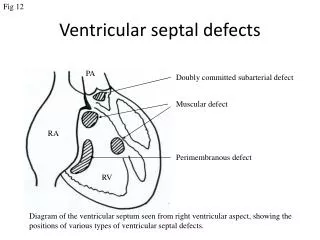
Anatomy of VSDs • Two types of VSD • Simple: through and through defect usually located anteriorly • Complex: serpentiginous dissection tract remote from the primary septal defect- most commonly an inferior VSD • Patient BG had such a presentation
Anatomy of VSDs • Antro-apical septal rupture • Comprise approximately 60-80% of cases • LAD occlusion is always the culprit
Anatomy of VSDs • Posterior septal rupture • Approximately 20-40% of cases • Occlusion of • Dominant RCA => extensive RV infarction • Dominant LCX (Less common), RV mostly spared
Anatomy of VSDs • Multiple defects (5-11% of cases) • Secondary to infarct extension • Evolve within days of each other
Anatomy of VSDs • Our series • Antro-apical septum Three of four cases • Posterior septum One of four cases
Pathophysiology • Antero-apical septal rupture • Tamponade • Secondary RV failiure due to acute volume overload
Pathophysiology • Posterior septal rupture • Commonly complicated by MR • Shunt reversal due to elevated RVEDP
Diagnosis • Loud/harsh pansystolic murmur • Within the first week post AMI • Best heard at Lt. Lower sternal border • Less loud at the apex • Associated with a palpable thrill • Depending on the location, may radiate to the axilla mimicking MR
Diagnosis • Up to 50% of patients experience chest pain associated with the development of murmur • CHF and shock often associated with the development of murmur
Diagnosis • Color Flow Doppler • 100% sensitive and specific in differentiating VSD from acute MR • Site of septal rupture correctly identified in 41 of 42 patients • One of our 4 patients had had a negative TTE earlier in the day, and no apparent homodynamic changes prior to the catheterization later that day Smyllie et. Al. 1990 JACC
Diagnosis Earlier diagnosis and surgical intervention, may be due to greater availability of Echocardiography at peripheral centers.
Diagnosis • Need for cardiac catheterization • 2/3 of the patients have multivessel coronary artery disease • Decreased operative mortality and improved late survival has been shown in patients with multivessel disease • Cardiogenic shock not a deterrent to Cath => Coronary angiography should be performed
Pre-Operative Management • Hemodynamic stabilization so as to minimize peripheral organ compromise • Reduce Systemic vascular resistance, and thus, the left-to-right shunt • Maintain or improve coronary artery blood flow • Maintain cardiac output and arterial pressure to ensure peripheral organ perfusion => IABP
Timing of Surgery • Controversial (in the past) • Non-randomized studies showing: • Early repair, 40% - 50% mortality • Late repair (past 3 weeks), 10% mortality => Aggressive Medical management aimed at delaying surgical intervention
Timing of Surgery • Short-coming of the argument Patients with less sever hemodynamic compromise, more likely to survive the acute phase without need for prompt surgery: Lower pre-op risk =>Better outcome
Timing of Surgery • Short-coming of the argument Patients with greater hemodynamic compromise, and more severe insult: Higher pre-op risk=>Worse outcome
Timing of Surgery • Surgery should be performed soon after diagnosis in most patients • Patients is cardiogenic shock should be operated on immediately after anigography • Hemodynamically stable patients should have surgery on an urgent basis
Operative Technique • Classical approach to antero-septal rupture • Infarctectomy, and • Reconstruction of the ventricular septum with Dacron patches
Operative Technique • Classical approach to infro-posterior rupture • Infarctectomy, and • Reconstruction of infroposterior VSD, • Reconstructionfree wall with Dacron patches.
Outcome • In a review of 139 cases reported in the literature prior to 1977 Six month survival without surgical intervention was less than 10%. Kirklin, Churchill Livingston 1993
Outcome • Predictors of early mortality per multivariable logistic regression analysis in a series of 22 patients • DM • Elevated RA pressure (RV involvement/IMI) • Absence of intraoperative IABP
Outcome • Predictors of early mortality per GUSTO analysis • Advanced age • Inferior location of MI
Outcome • In patients with cardiogenic shock mortality reported to be the highest • Posterior VSD (IMI) is another factor strongly associated with poor surgical outcome due to • Difficulty of exposure, and • Frequent concomitant infarction of the postero-medial papillary muscle Compilation from 6 series from the late 80s
Outcome • David, in a series of 44 patients reported no difference between mortality rates for the posterior and anterior VSD using the Exclusion technique
Exclusion Technique • Exclusion technique • LV excluded from the infarcted muscle using a bovine pericardial patch sutured to the healthy peri-infarct endocardium • No infarctectomy is performed • RV is undisturbed • Better RV function preservation • May help support the posteromedial papillary muscle
Exclusion technique Exclusion technique
Outcome • Residual Lt. Rt. shunt • Reported in up to 28% of survivors • Associated with high mortality • Intra-operative TEE useful in early detection and correction if deemed necessary • Seen in one of our patients. • Patient was treated medically
Post-Op state • Dialysis • Commonly required in patients in shock • Not required by either of our two survivors • Prolonged ventilatory support • Residual or recurrent VSD • Reoperation may be necessary depending on the shunt size and hemodynamics