Download
1 / 60
810 likes | 1.84k Views
Atrial Septal Defects. Imaging Conference 12/15/09 A. Zucker. Why do we care?. Most common congenital heart defect that presents during adulthood… We might have to diagnose it. Because we can fix it!!. Outline:. Embryology Types of ASD Presentation Shunts Echocardiographic evaluation

E N D
AtrialSeptal Defects Imaging Conference 12/15/09 A. Zucker
Why do we care? • Most common congenital heart defect that presents during adulthood… We might have to diagnose it Because we can fix it!!
Outline: • Embryology • Types of ASD • Presentation • Shunts • Echocardiographic evaluation • MRI • ASD closure
ASD • 10-15% of congenital heart defects • The 2nd most common congenital lesion found in adults (bicuspid aortic valve is the most common) • 1:1500 live births have an ASD • Male: Female ratio is 1:2 • Spontaneous closure is rare in children/ adults • Generally would have closed in infancy if it was going to close • Closure only seen in 4% of patients • Life expectancy is not normal, though many patients live to advanced age. • Natural survival beyond age 40-50 is <50%. • The attrition rate after age 40 is ~6% per year • First open heart closure of an atrialseptal defect (ASD) on September 5th, 1952
Embryology • Septation of the atria • Septum primum arises from the superior portion of the common atria and grows caudally towards the endocardial cushions. • Before the septum primum closes off the atria, it develops a fenestration called the ostium secundum. • The septum secundum arises from the right atrial side of the septum primum and grows caudally. • The septum secundum does not completely divide the atria and does not immediately fuse with the septum primum.
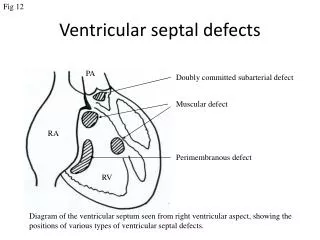
Types of ASDs Ostium Secundum Ostium Primum Sinus Venosus Coronary Sinus Defects
Secundum ASD • Most common type of ASD (70-75%) • ~7% of all congenital heart defects • Female predominance (2:1) • Includes all defects located in the area of the foramen ovales • Mechanisms of formation: • Septum secundum does not grow to cover the ostium secundum. • Ostium secundum is too large for the septum secundum to cover and so is left exposed despite a fully formed septum secundum.
Secundum ASD • Associatd findings: • MVP is present in 70% of pts with this type of ASD • Partial anomalous pulmonary venous connection (rare) • Specific EKG findings • Right atrial abnormality • Prolonged PR • Right axis deviation (>100 degrees) • rSR’ in v1 (incomplete RBBB) • Notching of R wave peak (“crochetage sign”)
Secundum ASD • rSR’ in v1 (incomplete RBBB) and notching of the R wave peak (“crochetage sign”)
Primum ASD • 15-20% of all ASDs • Female to Male ratio is 1:1 • Simplest form of AV canal defect • Generally associated with other anomalies • Commonly have AV valve defects, most notably a cleft in the anterior mitral valve leaflet • Defects of the ventriular septum • Common AV canal • Seen commonly in trisomy 21 • 40-50% of pts w/ Downs syndrome have CHD. Of these pts 65% are AV canal defects • Usually not a subtle finding
Primum ASD • Mechanism of formation: • Failure of the septum primum to fuse with the endocardial cushions (i.e. the ostium primum remains unclosed) • EKG findings: • PR prolongation • Right atrial enlargement • Left axis deviation • rSR’ (incomplete RBBB)
Primum ASD • Left axis deviation, rSR’ (incomplete RBBB), and PR prolongation
Sinus Venosus Defect • 1% of all congenital heat defects in the United States • Account for 10% of all ASDs • Not truly considered an ASD: • Abnormality in the insertion of the superior or inferior vena cava (which overrides the interatrial septum) • Two types: • Superior sinus venosus defects, located in the atrial septum immediately below the SVC • Inferior sinus venosus defects (less common), located in the atrial septum immediately above the IVC
Sinus Venosus Defect • Associated Findings • Both defects are often associated with a partial anomalous pulmonary vein connection with abnormal drainage • Pulmonary veins may be directed into the right atrium even if they are in the normal position • Pulmonary veins may also be completely displaced and insert into either vena cava • EKG changes • P wave negative in III and aVF and positive in Avl • Junctional/ low atrial rhythms
Coronary Sinus ASD • <1% of ASDs. • Mechanism of formation: • Loss of the common wall between the coronary sinus and the left atrium • Defect of at least a portion of the common wall separating the coronary sinus and the left atrium – AKA “unroofed coronary sinus” • Can be associated with a persistent left SVC draining into the coronary sinus
Shunting • Degree of shunt has implications as to whether to repair as ASD • Qp/Qs ratio correlates to the size of the ASD. • This falls apart when pulmonary hypertension is present • Repair of ASD when Qp/Qs (ratio of pulmonary flow to system flow) > 2:1 although some papers argue for 1.5:1 • AHA recommends >1.5:1, but this excludes individuals over 21 yrs of age • Canadian Cardiac Society recommends Qp/Qs >2:1, or >1.5:1 in the presence of reversible pulmonary hypertension • Recalculation of Qp/Qs every 2-3 yrs
Shunting • Decreased ventricular compliance +/- increased left atrial pressure lead to an increase in shunting • Decrease ventricular compliance: • Systemic hypertension • Cardiomyopathy • MI • Increase LA pressure • Mitral valve disease
Presentation • Often asymptomatic until the 3rd or 4th decade for moderate to large ASDs • Pts who present in infancy usually have associated cardiac defects • Fatigue • DOE • 30% by 3rd decade • 75% by 5th decade • Atrial arhythmias/ SVT and R sided HF: • 10% by 4th decade • Increases with age • Arrhythmias present in ~20% of pts
Presentation • Paradoxical embolus – stroke, TIA, or peripheral emboli: • Transient flow reversal secondary to increased R side pressures (valsalva) • PFO • Pulmonary hypertension • Migraine headaches: • PFO > ASD • Pulmonary hypertension: • Seen in less than 10% of pts w/ ASD at presentation • Seen in 50% of individuals above the age of 40. • Progression to Eisenmenger's syndrome occurs in 5 to 10% of individuals late in the disease process • Altitude intolerance • Increased decompression sickness and/or paradoxical emboli • Increased right to left shunting and decreased O2 saturations
Physical Findings • “Left atrialization” of JVP (A=V wave) • Hyperdynamic RV impulse • RV heave • PA tap • Split S1 • S2 wide/fixed split • Murmurs • Not hearing ASD (too little turbulance and too low velocity) • Systolic: • increased flow over pulmonic valve • Mitral regurgitation • Diastolic: • Pulmonary regurgitation due to PA dilatation • Increased flow across tricuspid valve
Echocardiographic Evaluation • Subcostal view most reliable: US beam perpendicular to plane of IAS • Other views may have loss of signal from the atrial septum from parallel alignment • Secundum ASD: central portion of atrial septum (89% sensitivity) • Primum ASD: adjacent to AV valve annuli (100% sensitivity) • Sinus Venosus defects: difficult to visualize on TTE (44% sensitivity)
Echocardiographic Evaluation • RV and RA size and function • Aids in evaluation of right to left shunt • Potentially the first abnormality noted on echocardiography • PW and CW Doppler to estimate RVSP and PA pressures • Drop-out of inferior portion of IAS can be seen on apical 4 or subcostal views • TV NOT more apically positioned than MV; at same horizontal level • Color to differentiate from dilated coronary sinus
Echo: • Identify: • Coronary sinus • Entrance of pulmonary veins • Primum portion of atrial septum • Drop-out of inferior portion of IAS can be seen on apical 4 or subcostal views • TV NOT more apically positioned than MV; at same horizontal level • Color to differentiate from dilated coronary sinus
Doppler Echocardiography • Color Doppler can identify left to right flow • Subcostal view is best • Multiple views needed: • Low-velocity flow signal between atria • SVC flow along IAS can be mistaken for shunting • TR jet directed toward IAS can also be confused as a shunt
Doppler Echocardiography • Location and timing of flow critical (as oppsed to the velocity) • Flow from L -> R atrium in both systole and diastole • More prominent diastolic component • Can extend across open TV in diastole into RV • Seen in larger shunts • Flow acceleration on side of LA • Absolute velocity of flow less important
Doppler Echocardiography • Shunt calculation: • Can be performed utilizing these equations to relate pulmonic CO and systemic CO • Qp = TVI pulm X PULd • Qs = TVI lvot X LVOTd • Qp/Qs = shunt fraction • Significant usually if > 1.5/1.0 in ASD
Constast Echocardiography • Microbubbles seen across IAS • Even if shunting predominantly L to R • RA pressure transiently > LA pressure • “Negative” contrast jet: • Flow from LA to RA appears as area with no echo contrast • Rarely needed for ASD - more useful for smaller shunts (PFO’s)
TEE • Needed when TTE images are suboptimal • Usually necessary to see sinus venosus defect or partial anomalous pulmonary venous return • To locate small secundum ASDs • Device sizing before percutaneousclosure • Estimation of defect size using the diameter of the Doppler color flow jet correlates with surgical findings • TEE is often used when contrast echo suggests shunting, but a defect can’t be visualized on TTE. The TEE then helps to differentiate between a PFO and a true ASD
MRI • Phase constrast MRI compares well against the gold standard (invasive measurement) • 93% sensitivity and specificity for Qp/Qs > or = 1.5:1 • 100% sensitivity and specificity for Qp/Qs > or = 1.7:1
MRI • Correlation of PC-MRI to TEE and IVBM (invasive balloon measurement) measurements of ASD size • Some studies have noted MR to have better correlation to balloon sizing of ASDs than TEE • MR also able to provide information about shape of ASD and proximity to adjacent structures • Possible that TEE will not be able to measure the largest section of the ASD if it is not round
ASD Closure • Percutaneous ASD closure was first performed 30 years ago • First report percutaneous ASD closure of via Amplatzer septal occluder in 1997 • Successful closure in >80% of secundum ASDs • Compared to surgical approach • Decreased LOS • Decreased complication rate • Same success rate • Determining factors: • Location • Size • <30 – 40 mm by TEE • Rim • Initial studies used rim of ~5mm in all directions • Some authors have proposed that it is the posterior inferior rim in particular that must be of adequate size for successful transcatheter closure
ASD Closure • Indications • Asymptomatic in the presence of: • Right-sided cardiac dilatation • ASD > 5mm with no signs of spontaneous closure • Hemodynamics reserved for “borderline” cases • HD insignificant (Qp/Qs <1.5) - no closure required until later in life for embolism prevention after CVA • HD significant (Qp/Qs >1.5) - should be closed • In presence of PA HTN: • Defined as PAP > 2/3 systemic or PVR > 2/3 SVR • Closure can be recommended IF: • Net L--> R shunt of 1.5:1 or greater • Pulmonary artery reactivity upon challenge with pulmonary vasodilator • Lung biopsy evidence of reversibility to pulmonary arterial changes
ASD Closure • Percutaneous indications: • Only for Secundum ASD with stretch diameter < 41 mm • Need adequate rims to enable secure device deployment • Cannot have anomalous pulm venous connection, be too proximal to AV valves, coronary sinus, or systemic venous drainage • ~2/3rds of secundum ASDs meet this criteria
ASD Closure • Introduced in 1996. • Approved for percutaneous ASD closure in 2001 by F.D.A. • Over 90,000 have been manufactured and delivered to date. • Consists of two round disks made of Nitinol (nickel + titanium) wire mesh linked together by a short connecting waist.
ASD Closure Amplatzer - advantages over other devices: • Can be delivered through smaller catheters • It is self-centering but can be repositioned easily • Has round retention disks that extend radially beyond the defect, which results in a much smaller overall size and firmer contact with the atrial septum • Shape enhances endothelialization and reducing the risk of residual shunting
ASD Closure • Complications of percutaneous closure: • Thrombus formation on the device leading to CVA • Decreased in newer devices • ASA and plavix after procedure for ~6 months • Heart block, effusion, and thrombus formation in LA (2.4%) • Device embolization and/ or malposition (2.4%) • Atrial fibrillation (2.4%) • Erosion (0.1%): • aortic to right or left atrial fistula • Free-wall perforation of the atria resulting in tamponade • Factors associated with erosion: • Amplatzer Septal Occluder size greater than 4 mm larger than the unstretched ASD • Device size greater than 1.5 times the size of the unstretched ASD