Download
1 / 38
400 likes | 915 Views
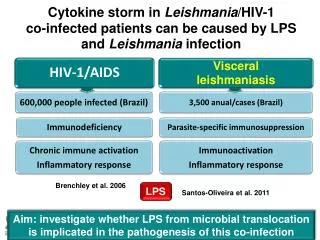
Tuberculosis and the Immune Reconstitution Inflammatory Syndrome (IRIS) . Bob Colebunders. Names. Immune reconstitution inflammatory syndrome (IRIS) Immune restoration disease (IRD) Paradoxical reactions. Pathogenesis.

E N D
Tuberculosis and the Immune Reconstitution Inflammatory Syndrome (IRIS) Bob Colebunders
Names • Immune reconstitution inflammatory syndrome (IRIS) • Immune restoration disease (IRD) • Paradoxical reactions
Pathogenesis • Increased lymphoproliferative response to mycobacterium antigens in vitro • Restoration of cutaneous response to Tuberculin • Increased [Il-6], activation markers (CD38) • Associated with TNFA-308*1, IL6-174*G
Incidence TB/IRIS Europe and USA • Narita et al 36% (Miami, 1998) • Wendel et al 11% (Baltimore 2001) • Breen et al 29% (London, 2004) • Breton et al 43% (Paris, 2004)
Incidence TB/IRIS Africa • Breton et al: 41% • No cases in TB/DOT study in South Africa (20 patients only) India • Kumarasamy et al: IRIS of 15.2 cases per 100 patient-years • Patel et al:TB IRIS more often in patients with active TB at the start of HAART than in those without active TB at the start of HAART (11 [8.73] vs. 3 [2.32%], respectively; p = 0.0489).
Risk factors for TB/IRIS • Starting ARV’s within 6 weeks of TB treatment • Disseminated, extra-pulmonary disease • Low base line CD4 count • Rise in CD4 % • Fall in viral load • High bacillary burden?
Types of TB IRIS • Patient unknown to have TB at the start of HAART • Patient on TB treatment before or at the start of HAART
Timing of IRIS • Mean of 15 days after starting HAART • Up to months (years) • Syndrome lasts for 10-40+ days
Prognosis • Breton et al: 16 cases of TB/IRIS: 5 ‘severe’ complications • Splenic rupture • Compressive lymphadenopathy • Ureteric obstruction • Narita et al: The study found a 6-fold increased risk of subsequent TB relapse in patients who experienced IRIS during early TB treatment.
Cryptococcal meningitis treated with HAART, bilateral blindness: fundoscopy: bilateral papiloedema: IRIS?
Differential diagnosis • Side effects of the antiretroviral treatment • Drug fever • TB infection not responding to standard anti-TB treatment • Other concomitant infection • Failure of HAART (late IRIS)
Proposed criteria for the diagnosis of IRIS in HIV patients on antiretroviral therapy French et al
Major criteria • Atypical presentation of ‘opportunistic infections or tumours’ in patients responding to antiretroviral therapy • Decrease in plasma HIV RNA level by 1log10 copies/mL
Minor criteria • Increased blood CD4 T-cell count after HAART • Increase in an immune response specific to the relevant pathogen, e.g. DTH response to mycobacterial antigens • Spontaneous resolution of disease without specific antimicrobial therapy or tumour chemotherapy with continuation of anti-retroviral therapy anti-retroviral therapy
“Suspected TB IRIS”: a TB patient who after starting HAART develops either • New persistent fevers (temperature >38.6°C) which last for more than 1 week without an identifiable source (e.g., urine and sputa testing, and other procedures when clinically indicated) or reason (e.g. an allergic reaction) • or marked worsening or emergence of intrathoracic lymphadenopathy, pulmonary infiltrates • or worsening or emergence of cervical adenopathies/abscesses, or worsening of other tuberculous lesions or manifestations, such as cutaneous peritoneal or central nervous system (CNS) inflammatory pathology.
“Suspected TB IRIS”: a patient who after starting HAART develops TB characterised bythe formation of • Large adenopathies • Abscesses • Miliary TB with large nodules • Cavity formation
“Confirmed” TB IRIS Same definition as suspected TB IRIS but • multi drug resistant TB excluded and • a satisfactory virological response to ART
Diagnostic investigations • AFB may be be present or absent • Viable organisms despite TB treatment since > 2 months may suggest treatment failure • Tuberculin skin testing • 88% of IRIS negative • 33% of non-IRIS negative
Recommendations to prevent TB IRIS • Exclude TB before starting antiretroviral therapy • Treat first the TB and start antiretroviral treatment only once the patient has clinically improved, is tolerating very well his TB treatment • Increase awareness about TB IRIS
Treatment recommendations • TB treatment should be continued • Exclude treatment failure • Ensure adequate treatment • Ensure adherence to ATT • Consider drug resistance
Treatment recommendations • Drainage • Adding prednisolone/NSAIDS may be beneficial • Continue HAART in most cases • Consider stopping ARV’s if life threatening?
Research questions? • Propose definition of IRIS • Validate clinical definition of IRIS • Incidence of TB IRIS in different populations? • Predictors/risk factors for IRIS? • Morbidity and mortality (cause of early deaths?) • What are the potential long term consequences?
How to diagnose TB IRIS? • What are the clinical manifestations of TB IRIS in adults and children? • Are there immunological markers or other simple laboratory parameters that could help to diagnose TB IRIS? • How useful is it to perform a tuberculin skin test prior to the start of ARVs and to repeat it when there is a suspicion of IRIS?
What is the pathophysiology of TB IRIS (early and late forms of IRIS)?
How to treat TB IRIS? Corticosteroids (dose, duration)?, NSAIDs? thalidomide?… Aspiration of abscesses? Should HAART be stopped? When? Should the management of early and late TB IRIS be different?
How to prevent/avoid IRIS? • When is the optimal moment HAART should be started in a HIV/TB co infected patient? • TB prophylaxis to avoid IRIS? • Corticosteriod therapy able to prevent the development of TB IRIS?
Operational issues • How to diagnose TB IRIS clinically at the primary health level? • When should a health care worker at the primary health care level refer a patient or call for advice?
Research methods • Cohort studies • Randomised clinical trials