Download

1 / 33
380 likes | 983 Views
TB-Associated Immune Reconstitution Inflammatory Syndrome (IRIS). John W. Wilson, MD Associate Professor of Medicine Division of Infectious Diseases Mayo Clinic, Rochester MN Mayo Clinic Center for Tuberculosis. Wisconsin TB Summit; April 24, 2014. TB-IRIS: General concepts.

E N D
TB-Associated Immune Reconstitution Inflammatory Syndrome (IRIS) John W. Wilson, MD Associate Professor of Medicine Division of Infectious Diseases Mayo Clinic, Rochester MNMayo Clinic Center for Tuberculosis Wisconsin TB Summit; April 24, 2014
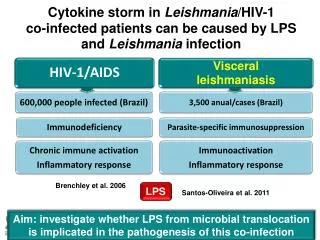
TB-IRIS: General concepts • The paradoxical worsening of signs, sx’s and/or radiologic features of TB after starting antiretroviral therapy (ART) for HIV infection • In setting of initial clinical improvement after starting TB-drug therapy • Incidence of TB-IRIS in HIV(+) patients is variable = 8-43% • Can occur in HIV (-) patients as well, but less common • E.g. CNS tuberculomas, cervical LNs Thorax 2004. 59:704-707 Clin Infect Dis 2006. 39:1709-12
Immunologic Reconstitution Inflammatory Syndrome (IRIS): principles - I Associated with increased functional immunologic & inflammatory responses - Examples: • HIV (+) patient: Recovery of CD4 T-cells after recent start of antiretroviral therapy (HAART, ART) • Leukemia, BMT patient: Recovery of neutrophils after myeloablative chemotherapy or hematopoietic stem cell transplantation (HSCT) engraftment • Solid organ trnplt pt: Reduction in pharmacologic immunosuppressive therapy
Immunologic Reconstitution Inflammatory Syndrome (IRIS): principles - II IRIS results from a rapid restoration of pathogen specific immune responses to opportunistic infections – causing either: • The deterioration of a treated infection via worsening symptoms, or • The new presentation of a previously subclinical infection Inflammatory response also augmented by increased MTB antigen loads released by dead or dying bacilli (AntivirTherap 2005, 10:417-22)
Immunologic Reconstitution Inflammatory Syndrome (IRIS): principles -III • Timing of IRIS onset: • During the first few months of ART • Generally sooner after myeloablative neutrophil recovery • IRIS can be associated with a wide array of pathogens - examples: • M. tuberculosis • Cryptococcus neoformans (e.g. meningitis) • Herpes viruses • IRIS not always limited to HIV (+) pts – e.g.: • Invasive filamentous fungal diseases (heme)
IRIS common with other HIV-associated opportunistic infections Meta-analysis of immunologically advanced HIV (+) ptsdeveloping IRIS after starting ART: • 13,100 pts among 54 cohort studies Incidence of IRIS s/p ART start: • Cytomegalovirus (CMV) – 37.7% • Cryptococcus meningitis – 19.5% • PML – 16.7% • Tuberculosis 15.7% • Herpes zoster – 12.2% • Kaposi's sarcoma – 6.4% Müller et al. Lancet Inf Dis 2010;10:251-61
CNS VZV–IRIS (non-TB) • 37 yo HIV (+) woman with VZV lesions - T7 dermatome • Treated with acyclovir 6 weeks prior to admission • HAART was initiated 2 weeks PTA • Double vision was followed by severe weakness in her legs 1–2 days PTA Post el at. Am J Neuroadiol. 2013 Jul;34(7):1308-18
IRIS common with other HIV-associated opportunistic infections - II Deaths in patients developing IRIS: • 20.8% in pts with cryptococcal meningitis • 3.2% pts in pts with TB • Lower CD4 counts at time of ART start – associated with high risk of IRIS • Especially when CD4 < 50 cells/uL Müller et al. Lancet Inf Dis 2010;10:251-61
Distinguishing between:1 - TB-associated IRIS and 2 - ART-associated TB Meintjes et al. Lancet Infect Dis 2008; 8: 516–23
Diagnosing TB-associated IRIS • *No single laboratory or confirming test for TB-IRIS • IRIS is a clinical diagnosis – based on • Timing of TB and/or HIV therapies and case definitions • Clinical signs, pt. symptoms with supportive radiologic studies and laboratory information • Underlying risk & predisposing patient factors towards IRIS (e.g. low CD4 before starting ART) • Must exclude other diagnoses including: • Other opportunistic or community-based infections • Negative tissue stains, cultures, PCR; serologies, etc. for alternative pathogen(s) • Aseptic causes of inflammation • Malignancies • Other processes
Symptoms and Clinical findings of TB-IRIS- can be quite variable - I • Clinical examples: • New or recurrent fever (may be most common) • New or recurrent cough • New or worsening lymphadenopathy • New skin lesions • New soft tissue abscess • New or recurrent seizure (e.g. CNS tuberculoma)
Symptoms and Clinical findings of TB-IRIS- can be quite variable - II • Radiologic examples: • New intraabdominal adenopathy • New pulmonary infiltrate • *Worsening CXR infiltrate → can still be IRIS; but must r/o drug-resistant TB or non-TB cause • New pleural effusion
Paradoxical TB-associated IRIS 36 yo HIV (+) pt; baseline CD4 of 39 cells with culture (+) pulmonary TB Cervical LN enlargement (1 week after starting ART) Chest wall cold abscess Right psoas abscess (CT scan) Worsening cough with sputum AFB staining (+); but culture (-) Meintjes et al. Lancet Infect Dis 2008; 8: 516–23
Presentations of miliary TB-IRIS after starting HAART A. Miliary Pulmonary TB C. Cerebral tuberculomas with meningeal TB D. Choroid tubercles Sharma et al. Indian J Med Res 135, May 2012, pp 703-730
Presentations of miliary TB-IRIS after starting HAART Sharma et al. Indian J Med Res 135, May 2012, pp 703-730
Timing of TB-IRIS onset • Generally presents within the first 3 months • Usually within the first 2 months or even first few weeks after starting ART Bangkok, Thailand: 167 patients 21 (12.6% developed TB- IRIS) Journal of Infection (2006) 53:357-63
Case definition for paradoxical TB-IRIS - 3 components to case definition: Lancet Infect Dis 2008;8(8):516-523
ART-associated TB “Unmasking” tuberculosis-associated IRIS 48 yo HIV (+) pt; baseline CD4 of 10 cells with dry cough (no sputum collected) Baseline CXR clear 10 days after starting ART – (+) fever and worsening productive cough. Sputum (+) AFB The rapid development of pulmonary symptoms and infiltrated attributed to the ‘unmasking of TB-associated IRIS Chest wall cold abscess Meintjes et al. Lancet Infect Dis 2008; 8: 516–23
Case definition for ART-associated TB - 3 components to case definition: • Patient is not receiving TB treatment when ART is started • Active TB has not yet been diagnosed (when ART started) • Active TB is diagnosed after ART has been started • Diagnosis of TB should meet WHO criteria for AFB smear (+), smear ()-) or extrapulmonary TB Lancet Infect Dis 2008;8(8):516-523 Case Rep Infect Dis. 2013; 2013:1-7
Presentations of ART-associated TB- “unmasking” IRIS • Pulmonary TB most common • Other sites periodically encountered: • Spinal TB • Spondylodiscitis • Paraspinal abscess(s) – in up to 50% cases • Psoas abscess • AFB stains and cultures may be positive – e.g. • Sputum – pulmonary source • Needle aspiration • Tissue biopsies Case Rep Infect Dis. 2013; 2013:1-7
Risk factors for TB-associated IRIS development in HIV (+) pts: • Baseline low CD4 cell count (e.g. CD4 < 100 cells/uL) • Rise in CD4 count with effective ART during first 3 months of therapy • Disseminated TB (extrapulmonary TB) • More common in advanced HIV (+) pts • Earlier start of ART • Balancing potential reductions in AIDS-related mortality risk vs. IRIS morbidity & mortality risks • No effect on IRIS • Latent TB infection (much lower MTB load) - ↓↓ risk (if any) • Type if ART therapy used Michailidis et al. AntivirTherap2005, 10:417-22
Associations between pre-ART clinical and laboratory characteristics with subsequent TB-IRIS events Narendran et al. PLoSOne. 2013; 8(5): e63541
Pre-ART plasma levels of IL-6 or CRP distinguish individuals at higher risk for TB-IRIS Narendran et al. PLoSOne. 2013; 8(5): e63541
Not every HIV-TB pt with low CD4 cell counts develops TB-IRIS Reasons for such discordance among patients is not overly clear - examples: • Complex interplay of immune responses and/or severity of immunosuppression • Inter-patient genetic predisposition • E.g. humoral immune response – abnormalities in IL-12 and IFN-γ • Higher MTB bacilli burden; antigen load • E.g. rise of antigen release after treatment started • Anatomic location of MTB infection • Other??
When to start HIV antiretroviral therapy (ART) in patient with active TB?Considerations: CurrOpin HIV AIDS. Jan 2010; 5(1): 61–69
Early vs. Late introduction of ARTCAMELIA study (Cambodia) • Patients who had CD4 counts <200 cells/mm3 were randomized to initiate ART at 2 wks or 8 wks after start of TB treatment. • Enrolled pts with advanced HIV disease, median CD4 of 25, low BMI, high rates of disseminated TB • Compared with ART started at 8 wks, ART started at 2 wks resulted in a 38% reduction in mortality (P = 0.006) N Engl J Med. Oct 20 2011;365(16):1471-1481
Early vs. Late introduction of ARTCAMELIA study (Cambodia) • However, pts starting ART earlier (at 2 weeks) had a higher incidence of IRIS (36%) compared to pts starting ART at 8 weeks (16%) • Most frequent IRIS findings: • Progressive adenopathy • Fever • Abdominal pain • HSM • TB-assoc. IRIS was very manageable • Low mortality (3.9%) Laureillard et al. AIDS 2013, 27:2577–2586
CAMELIA Trial: Kaplan–Meier estimates of occurrence of TB-associated IRIS by study arm Laureillard et al. AIDS 2013, 27:2577–2586
The ACTG 5221 (STRIDE) trial • Multinational study, randomized ART-naive patients with confirmed or probable TB and CD4 counts <250 cells/mm3 • Earlier (<2 weeks) ART or later (8–12 weeks) ART • Overall rates of mortality and AIDS diagnoses were not different between the earlier and later arms – However: • Higher rates of IRIS were seen in the earlier ART arm • Asignificant reduction in AIDS or death was seen in the subset of patients with CD4 <50 cells/mm3 who were randomized to the earlier ART arm Havlir et al. N Engl J Med. Oct 20 2011;365(16):1482-1491
Basic TB and HIV Treatment Principles – Summary (DHHS) • All HIV-infected patients with diagnosed active TB should be started on TB treatment immediately (AI) • TB has the priorityin timing • All HIV-infected patients with diagnosed active TB should be treated with antiretroviral therapy (ART) (AI) • Timing of starting ART depends upon patient factors, including: • CD4 count • Clinical severity of HIV disease 2013 DHHS Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescentshttp://aidsinfo.nih.gov/guidelines on 4/14/2014
Basic TB and HIV Treatment Principles – Summary (DHHS) – II • In ptswith CD4 counts <50 cells/mm3, ART should be initiated within 2 weeks of starting TB treatment (AI) • In pts with CD4 counts ≥50 cells/mm3 who present with clinical disease of major severity (e.g. low Karnofsky score, low body mass index, low Hgb, low albumin, organ system dysfunction, etc), ART should be initiated within 2 to 4 weeks of starting TB treatment • Strength of this recommendation varies on the basis of CD4 cell count: • CD4 count 50 to 200 cells/mm3 (BI) • CD4 count >200 cells/mm3(BIII) 2013 DHHS Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents http://aidsinfo.nih.gov/guidelines on 4/14/2014
Basic TB and HIV Treatment Principles – Summary (DHHS) – III • In ptswith CD4 counts ≥50 cells/mm3 who do not have severe clinical disease, ART can be delayed beyond 2 to 4 weeks of starting TB therapy but should be started within 8 to 12 weeks of TB therapy initiation. • The strength of this recommendation also varies on the basis of CD4 cell count: • CD4 count 50 to 500 cells/mm3 (AI) • CD4 count >500 cells/mm3 (BIII) • In all HIV-infected pregnant women with active TB, ART should be started as early as feasible, both for maternal health and for prevention of mother-to-child transmission (PMTCT) of HIV (AIII) • In HIV-infected patients with documented MDR- or XDR-TB, ART should be initiated within 2 to 4 weeks of confirmation of TB drug resistance and initiation of second-line TB therapy (BIII) 2013 DHHS Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents http://aidsinfo.nih.gov/guidelines on 4/14/2014
The End Questions?