Download

1 / 22
220 likes | 761 Views
Progressive Degenerative Communication Disorders of Older Adults: Incidence, Pathology , Treatment Practical Clinical Consideration in the Healthcare Setting. Faerella Boczko, M.S.,CCC-SLP, BRS-S Board Recognized Specialist in Swallowing and Swallowing Disorders

E N D
Progressive Degenerative Communication Disorders of Older Adults: Incidence, Pathology, Treatment Practical Clinical Consideration in the Healthcare Setting Faerella Boczko, M.S.,CCC-SLP, BRS-S Board Recognized Specialist in Swallowing and Swallowing Disorders Director of Speech – Language Pathology Jewish Home and Hospital Lifecare System Bronx, New York
General Characteristics of Speech • Monopitch (breathy, hoarse, vocal quality) • Monoloudness (decrease in loudness level) • Increase of rate • Reduced stress • Short rushes of speech with imprecise articulation of consonants • Inappropriate sentences (may be related to bradykinesia) • Difficulty initiating movements for speech
General Communication Strategies • Increase respiratory support, erect posture, take a deep breath before speaking, increasing effort during speech (to increase loudness) • LSVT ( to increase phonatory effort) • Delayed auditory feedback • Voice amplification • Strategies to increase vocal fold adduction (to improve breathy hoarse vocal quality) • Slow rate, overarticulation (to improve imprecise articulation and short rushes of speech)
Communication Strategies (cont’d) • Increase empatic stress patterning • Exaggerate loudness • Exaggerate stress patterns, emphasize various consonants • Computerized software programs-visipitch • Augmentative communication systems-alphabet board (identify first letter), pacing board (touch a square-say a word-individuals with palilalia), portable typing device, picture book (need to be aware of movements becoming automatic-festination pattern).
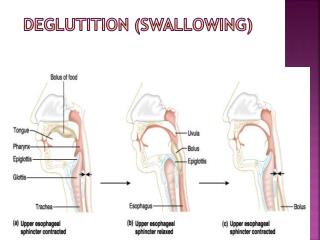
General Swallowing Difficulties • Slow oral transit time • Tongue pumping • Decrease in tongue movement/difficulty with propulsion and A-P transport of the bolus • Drooling • Lingual tremor • Piecemeal deglutition
Swallowing Difficulties (cont’d) • Bolus falling out of the oral cavity • Delay in the initiation of the swallow • Decrease in pressure generation during the swallow • Decrease in laryngeal elevation • UES dysfunction • Increase risk of aspiration during and after the swallow
General Swallowing Strategies * (based on a comprehensive assessment and based on the physiology of the individuals swallow) Compensatory techniques • Postural changes such as chin tuck; upright 60-90 degrees during and following oral intake; may use air filled back pillows and/or body positioners • Improving sensory awareness: increasing taste, alternating temperature and flavor (sweet-sour) • Diet modification-may need to change diet consistency to soft or puree or change the liquid consistency. May need to allow extra time to swallow. May need to verbally cue patient to take small bites and think “swallow.” • Consult with occupational therapy to provide assistive feeding devices/eating utensils to maintain self-feeding. These could include: a wonder flo cup, two handle cup, dysphagia cup, sure grip utensils, partition plate, scooper bowls, ez grip utensils, or Dycem nonslip plastic. • Provide high caloric frequent meals/snacks. Use finger type foods.
General Swallowing Strategies Rehabilitative techniques • Swallowing maneuvers ( Mendolsohn maneuver, supraglottic swallow, super-supraglottic swallow) • Resistance exercises • Vocal adduction exercises • Laryngeal elevation exercises • Isometric and isokinetic exercises (Shaker exercise) • PEG- percutaneous gastrostomy- alone or may combine with some oral intake and supplement tube feeding
General Speech Characteristics • Slow, laborious production of words/short phrases with defective articulation that at times is unintelligible • Hypernasality-air escaping through the nose-inability to build up intraoral air pressure-nasalization of vowel sounds • Changes in prosody with monotonous quality (long pauses between words and phrases) • Inability to adduct vocal folds and phonate-breathiness,hoarseness,wet /gurgly quality
General Communication Strategies *(In general avoid oral motor exercises-no research and no evidence to suggest that these exercises will improve speech production and may cause fatigue) • Minimize environmental distractions. Reduce background noise -T.V./radio should be off when attempting to communicate. • Take the patient to a quiet area to communicate. Face the patient. • Introduce your topic of conversation so that the patient can focus on the topic. • Stay in close proximity with the patient so that the patient can conserve energy and have sufficient respiratory support to speak. • Encourage the patient to use a slow and exaggerated manner of speaking • Patient may need to be referred for a palatal device/prosthetic device to compensate for loss of air through the nose
General Communication Strategies(cont’d) • May need a speech generating device: • Augmentative system - alphabet board (point to the first letter of each word) • Spelling • Writing systems • Bells/ringing device to alert an individual in another room • Yes/no/I don’t know system - head nods, eye movements
General Swallowing Characteristics • Food spillage and drooling (may be related to lip weakness) • incoordination of buccal muscles, the tongue and the palate resulting in inability to initiate swallow • Inability to gather saliva in oral cavity and move the bolus to the back of the oral cavity • Weakness of soft palate causing ineffective transport of food • Decrease in pressure generation and decrease in propulsive force to move the bolus into the larynx and into the esophagus • Weakness in pharyngeal constrictors • Accumulations of secretions in the larynx • Evidence of decrease in food intake, dehydration, weight loss • Respiratory weakness varies and should be noted and assessed in terms of depth and volume of respiration and cough force (can use a hand held respirometer to assess vital capacity)
General Swallowing Strategies * (must be based on a comprehensive assessment when physiological disorders are identified. Management and treatment of dysphagia involves knowledge of the underlying neurophysiologic and biomechanical principles of swallowing function and identification of any deviation from the normal swallowing pattern). Techniques are compensatory and do not include rehabilitative techniques - • Postural changes-upright position while and after eating; chin tuck position • Verbal cues to provide double swallows to clear oral cavity • Sensory stimulation-increase taste, alternate food temperature and flavor • Modification of the feeding/eating process such as changes in the food and liquid consistency and allowing extra time to swallow • Increase liquid intake (to decrease possibility of dehydration and thickened salivary secretions) by providing snacks and items such as sherbert, frozen fruit pops
Speech and Swallowing Characteristics • Phonatory disturbances • Rapid rate of speech • Choreic movements • Rapid uncontrolled swallowing (tachyphagia) • Delay in the initiation of the swallow • Impaired mastication, segmented and delayed lingual transport of the bolus • Eructations (excessive belching) • Choking, coughing, wet vocal quality
General communication strategies • Chewing, yawning, relaxation techniques • Prosody drills • Augmentative communication systems - alphabet boards, yes/no system, memory aids • Postural changes-reduce hyperextension of the neck and trunk by providing rubber wedge; promote chin tuck position • Eating modification-adaptive devices may be needed • Provide frequent high caloric snacks; finger foods; increase calories by adding extra butter, cream • Modified supraglottic swallow-swallow-cough-swallow • Alternative means of hydration and nutrition General swallowing strategies
Speech and Swallowing Characteristics • Weakness, fatigue, spasticity, incoordination, ataxia, tremor, dysmetria • Impaired control of loudness, harshness, defective articulation, impaired pitch control, hypernasality • Vocal tremor, harsh voice, reduced speaking rate (worsens with fatigue) • Abnormal speech breathing behaviors (may initiate phonation at inappropriate lung volume levels, speech either excessively loud or quiet; does not terminate breath group at appropriate lung volume level)
General communication strategies • Teach energy conservation techniques • Teach loudness regulation techniques • Teach appropriate respiratory patterns • Eliminate abnormal respiratory behaviors such as inhaling too deeply and then exhaling most of the air before speaking or taking a breath only after they have completely run out of air • Paced speech (visipitch) • Respiratory patterns-rate control, use appropriate phrasing and breath patterning • Supplement with speech and alphabet board (point to first letter of each word)
General swallowing strategies(compensatory) • Minimize environmental distractions • Postural changes (upright, chin tuck) • Modification of the feeding/eating process-increase attention on the act of eating and swallowing, increase taste and flavor, alternate temperature • May need to thicken liquids • May need to consider alternate means of hydration and nutrition