Download
1 / 88
970 likes | 2k Views
Cohort Study. Subodh S Gupta Dr. Sushila Nayar School of Public Health MGIMS, Sewagram. Origin of word ‘cohort’. The word ‘cohort’ has its origin in the Latin ‘ cohors ’ ‘ cohors ’ (Latin word) = Refers to warriors and gives notion of a group of persons proceeding together in time

E N D
Cohort Study Subodh S Gupta Dr. Sushila Nayar School of Public Health MGIMS, Sewagram
Origin of word ‘cohort’ • The word ‘cohort’ has its origin in the Latin ‘cohors’ • ‘cohors’ (Latin word) = Refers to warriors and gives notion of a group of persons proceeding together in time • Group of persons with a common statistical characteristic; e.g. age, birth date
Definition & Synonyms Definition “The cohort study is an observational epidemiological study which, after the manner of an experiment, attempts to study the relationship between a purported cause (exposure) and the subsequent risk of developing disease.” Synonyms • Follow-up • Longitudinal • Prospective • Incidence study
The cohort design • Groups are exposure based:The group or groups of persons to be studied… are defined in terms of characteristics manifest prior to the appearance of the disease under investigation • The study is conceptually longitudinal: The study groups so defined are observed over a period of time to determine the frequency of disease among them • A definite beginning and end
The cohort design • Efficient for examining • When there is good evidence of exposure and disease. • When exposure is rare but incidence of disease is higher among exposed • When follow-up is easy, cohort is stable • When ample funds are available • Common outcomes
The cohort design • Many different outcomes for same exposure • The dynamic nature of many risk factors and their relations in time to disease occurrence can be captured here (cannot be done in cross-sectional study and only with difficulty in case-control study) • Associations (not cause and effect) • Estimate incidence within risk factor groups • Cannot estimate prevalence of risk factor
Population Exposed Cases (People with disease) Not exposed Exposed Controls (People without disease) Not exposed Time Case control study Direction of enquiry
Population Diseased Exposed Not diseased People without the outcome Diseased Not Exposed Not diseased Time Cohort study Direction of enquiry
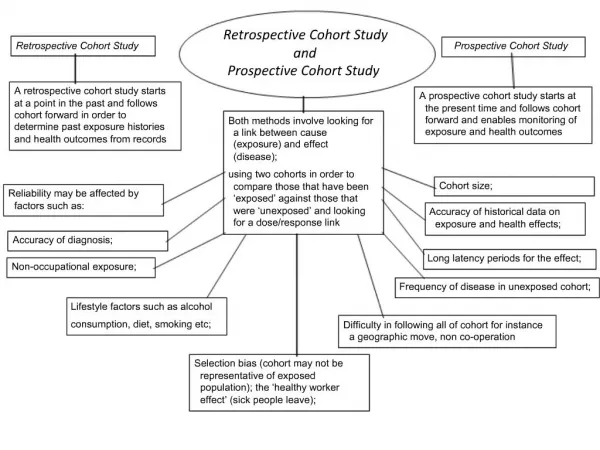
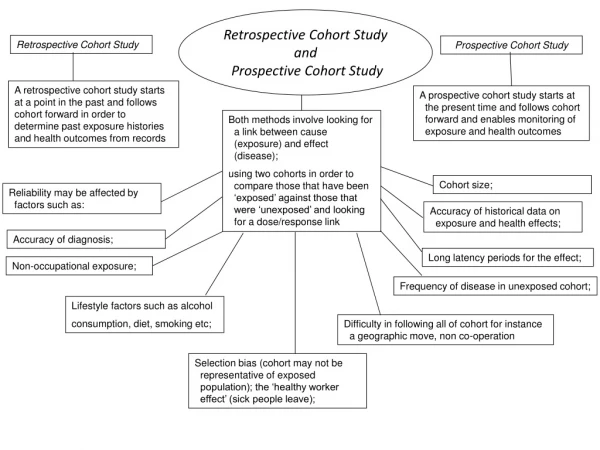
Types of cohort study • Historical/ Retrospective/ Non-concurrent • Prospective/ Concurrent The distinction between retrospective and prospective cohort studies is important, not because of any conceptual difference or differences in interpretability of findings, but because of relevance to some practical issues, mostly the ability to control confounding.
Population Diseased Exposed Not diseased People without the outcome Diseased Not Exposed Not diseased Time Point in time when enquiry begins? Direction of enquiry
Population Diseased Exposed Not diseased People without the outcome Diseased Not Exposed Not diseased Time Both exposures and outcomes measured prospectively Direction of enquiry
Population Diseased Exposed Not diseased People without the outcome Diseased Not Exposed Not diseased Exposures measured retrospectively and outcomes prospectively Time Direction of enquiry
Population Diseased Exposed Not diseased People without the outcome Diseased Not Exposed Not diseased Both exposures and outcomes measured retrospectively Time Direction of enquiry
Advantages • Direct estimate of risk and rate of disease occurrence over time • An efficient means of studying rare exposures • Assess multiple outcomes of a single exposure • Establish temporal relationship between exposure and outcome • Exposure definitely precedes the outcome • Avoids recall bias, survival bias • Does not require strict random assignments of subjects • Can be done with original data or secondary data Best observational design to establish association
Disadvantages • Very large sample sizes, especially for rare outcomes • Expensive and time-consuming • Attrition problem (Loss to follow-up) • Differences in the quality of measurement of exposure or disease b/w the cohorts may introduce misclassification (information bias) • Can not infer causal relation • Very specific finding • Complexity of data analysis • Ethical issues • Study effects
Alternate designs and concerns • Two separate cohorts; exposed and unexposed subjects • Omission of non-factor group • Use of external comparison • Use of mortality than morbidity as outcome • Event notification arises from routine statistics, rather than special observations • Comparison of several groups • Competing causes of death
Steps in conducting cohort study • Identification of study population and initial steps • Measurement of exposure • Selection of study and comparison cohorts • Follow-up (for outcome measurement) • Data analysis
Types of cohorts • Closed or fixed cohorts: • Fixed group of persons followed from a certain point in time until a defined endpoint • Starting point - exposure defining event Endpoint – occurrence of the disease, loss to follow-up, death • The exposure is an event which occurs only once • Open or dynamic cohorts: • Subjects may enter or leave the study at any time • Exposure status may change over time
Cohorts • General population cohorts: population groups offering special resources for follow-up or data linkage are chosen, and the individuals are subsequently allocated according to their exposure status • Special exposure cohorts: Samples chosen on the basis of a particular exposure Exposures may be a particular event, a permanent state or a reversible state
General population cohorts (groups offering special resources) • Groups with readily available health records • Certain professional categories • Obstetric populations • Volunteer groups • Geographically identified cohorts • Record linkage
Special exposure cohorts (groups offering special resources) • Exposed to certain factor or event • Occupational groups • Based on qualitative characteristics
Population-based Cohort Studies Advantages • Estimation of distributions and prevalence rates of relevant variables • Risk factor distributions • Ideal setting in which to carry out unbiased evaluation of relations
Selection of comparison group • Internal comparison • Only one cohort identified • Later on, classified into study and comparison cohort based on exposure • External comparison • More than one cohort identified • e.g. Cohort of radiologist compared with ophthalmologists • Comparison with general population rates • If no comparison group is available we can compare the rates of study cohort with general population • Cancer rate of uranium miners with cancer in general population
Ideal Cohort • Stable cohort • Cooperative cohort • Committed cohort • Well informed cohort
Exposure measurement • Exposures: exogenous and/ or endogenous • Reference period • Frequency of follow-up • Challenge of prospective data collection • Changes in instrument over time • Use of repeated measures • Data collection costs
Sources of information • Records • Cohort members: self-administered questionnaires, interviews, telephone interviews, mailed questionnaires, • Medical examination & biomarkers: Clinic examinations & lab tests • Measures of the environment: level of air pollution, quality of drinking water, airborne radiation • Multiple methods
Follow-up: Types of outcomes Discrete events • Single events • Mortality • First occurrence of a disease or health-related outcome • Multiple occurrences • Disease outcome • Transition between states of health/ disease • Transitions between functional states • Level of a marker
Exercise 1 • An investigator wants to discover whether or not being overweight in adolescence increases the risk of cardiovascular mortality in adulthood. • Assuming historical records are available, would a prospective or retrospective study be more practical? • Who would comprise the investigator's cohort under study? • Who would comprise the investigator's exposed and unexposed groups in this cohort?
Group Exercise Design a Cohort Study Outline the steps which you will require to do for this study Special efforts you may need to do for follow-up of the study subjects What care you will need to take to reduce measurement bias Calculate the sample size
Age Calendar period Exposure 1 Exposure 2 Exposure i Covariate 1 Covariate 2 Covariate i Start of study End of study Challenge 1:multiple dimensions of time in cohort study
Challenge 2:Retaining cohort study members • Loss to follow-up • Dropouts • Can not be traced • More concern: those who cannot be traced; May have moved because they have developed the disease
Effect of Nonresponse • Nonresponse: a major problem • A differential nonresponse will distrorts the true relationship b/w exposure and outcome
Nonresponse: random or selective? • Exposure data: find out if nonrespondents are different from the respondents • Intensive efforts within the study design • Follow-up of the nonrespondents as well as respondents
Challenge 3:Large Modern Cohort Studies • Huge requirements of resources and manpower • Management of huge database • Follow-up • Exposure information • Data quality? • Collection of biologic samples?
Challenge 4:Long term follow-up • Operational problems • Cumulative risk getting closer to one
Two types of measures for rate • Cumulative incidence = Proportion of study subjects getting the outcome during the study period • Incidence rate = New cases/ Person-time under observation
1. Cumulative incidence rate: Number of new cases of disease occurring over a specified period of time in a population at risk.
EXAMPLE A surveillance system for Hospital acquired infection among the post-operative patients in a month.
Example 9 6 14 14 24 19 14 4 5 19 21 6 0 5 10 15 20 25 30
2. Incidence density: Number of new cases of disease occurring over a specified period of time in a population at risk throughout the interval.
Incidence density requires us to add up the period of time each individual was present in the population, and was at risk of becoming a new case of disease. Incidence density characteristically uses as the denominator person-years at risk. (Time period can be person-months, days, or even hours, depending on the disease process being studied.)
USES OF INCIDENCE DENSITY AND CUMULATIVE INCIDENCE • Incidence density gives the best estimate of the true risk of acquiring disease at any moment in time. • Cumulative incidence gives the best estimate of how many people will eventually get the disease in an enumerated population.
Comparing risks in different groups • Relative risk OR Risk ratio (RR) • Attributable risk OR Risk difference (AR) • Attributable risk percent (AR%) • Population attributable risk (PAR) • Population attributable risk percent (PAR%) • Odds Ratio (OR)