Download
1 / 26

E N D
1. Educating and empowering frontline staff to recognise and respond appropriately to the deteriorating patient John Lewandowski
Clinical Educator Team Leader
My name is John Lewandowski and I lead a team of educators in our Trust who are responsible for rolling out the NICE competencies for acute illness across our two sites. This presentation will cover how we did that
This is only a small and specific part of an overall Trust strategy to reduce mortality (e.g. Infection control, nutrition, medication safety, falls, tissue viability and so on). However, our role and that of the competencies does overlap with many of these inititiatives
This slide set may have some slight changes from the one in your pack so just be aware
My name is John Lewandowski and I lead a team of educators in our Trust who are responsible for rolling out the NICE competencies for acute illness across our two sites. This presentation will cover how we did that
This is only a small and specific part of an overall Trust strategy to reduce mortality (e.g. Infection control, nutrition, medication safety, falls, tissue viability and so on). However, our role and that of the competencies does overlap with many of these inititiatives
This slide set may have some slight changes from the one in your pack so just be aware
2. This bold target was set back in 1998
And I want to show you how we have been and still are part of that
I will cover three broad themes of how we moved forward
This bold target was set back in 1998
And I want to show you how we have been and still are part of that
I will cover three broad themes of how we moved forward
3. Overview You cant deliver competencies without a supportive framework and that�s the first point I will explore
Co-ordinated strategy �essential in facilitating the way for success in competency development and delivery
Without clinical leadership, staff support and correct underlying mechanisms and processes, then the educational principles that are laid out in the competencies will not necessarily be adopted by front line staff and staff will not be empowered
2. Developing & assessing competence in practice
Second point is the nuts & bolts of how competencies (Drawn from NICE 50) were drawn up and delivered across our Trust.
3. Competence and practice development
The third thing to explore will be to highlight that you cant have competencies without supportive practice development
and the compliance of ward staff and managers. Its not just about jumping through hoops. Staff can see the link between competencies and policy
So, focusing on the first element...
You cant deliver competencies without a supportive framework and that�s the first point I will explore
Co-ordinated strategy �essential in facilitating the way for success in competency development and delivery
Without clinical leadership, staff support and correct underlying mechanisms and processes, then the educational principles that are laid out in the competencies will not necessarily be adopted by front line staff and staff will not be empowered
2. Developing & assessing competence in practice
Second point is the nuts & bolts of how competencies (Drawn from NICE 50) were drawn up and delivered across our Trust.
3. Competence and practice development
The third thing to explore will be to highlight that you cant have competencies without supportive practice development
and the compliance of ward staff and managers. Its not just about jumping through hoops. Staff can see the link between competencies and policy
So, focusing on the first element...
4. 1: Coordinated & Supportive Strategy Strong clinical leadership is the first of three aspects I would like to discuss regarding our co-ordinated and supportive strategy
Our Trust has a strong board to ward philosophy to enhance clear lines of communication and responsibility. Mechanisms to reflect this include:
Quarterly reports
We have a greater interface between board and ward with a much greater focus on quality which is taken very seriously
QR include key information on falls, pressure sores, clinical incidents, complaints, clostridium difficile and MRSA. EWS audits included. Some discussion at the moment of adding chart checker (PDSA) and whether we should add cardiac arrest rates
2. LIPS � leading improvement in patient safety
We have a patient safety lead who is engaging re: patient safety first as well as GTT mortality reviews & trigger events = adverse incidents (e.g. Lack of EWS, return to theatre, arrest etc)
3. Patient Safety First Campaign
The work undertaken by my team has been supported by the wider work going on to reduce harm as part of the Patient Safety First Campaign which the Trust is actively participated in. We have a patient safety lead for LIPS who engages with this
4. QRP � example on the next slide
Our nursing director is an active lead for the QRP � doing the rounds etc
5. Also:
We have a steering group for acute illness
Strong clinical leadership is the first of three aspects I would like to discuss regarding our co-ordinated and supportive strategy
Our Trust has a strong board to ward philosophy to enhance clear lines of communication and responsibility. Mechanisms to reflect this include:
Quarterly reports
We have a greater interface between board and ward with a much greater focus on quality which is taken very seriously
QR include key information on falls, pressure sores, clinical incidents, complaints, clostridium difficile and MRSA. EWS audits included. Some discussion at the moment of adding chart checker (PDSA) and whether we should add cardiac arrest rates
2. LIPS � leading improvement in patient safety
We have a patient safety lead who is engaging re: patient safety first as well as GTT mortality reviews & trigger events = adverse incidents (e.g. Lack of EWS, return to theatre, arrest etc)
3. Patient Safety First Campaign
The work undertaken by my team has been supported by the wider work going on to reduce harm as part of the Patient Safety First Campaign which the Trust is actively participated in. We have a patient safety lead for LIPS who engages with this
4. QRP � example on the next slide
Our nursing director is an active lead for the QRP � doing the rounds etc
5. Also:
We have a steering group for acute illness
5. Quality Review Sharing good practice � how do we feed back and share the results? Well, this is one of the other themes for having a co ordinated and supportive strategySharing good practice � how do we feed back and share the results? Well, this is one of the other themes for having a co ordinated and supportive strategy
6. 1: Coordinated & Supportive Strategy Share Good practice/Recognition and Performance
Why does it work and what works? e.g. Learning from and within other teams (e.g. QRP, stop the clock/non essential tasks)
2. Take responsibility
e.g. Linked to acute competencies part of KSF
3. Learn from patients
e.g. key component of QRP. Incident reporting & action planning. Direct link to the CLIP report (complaints & litigation, incidents, PALS). Case discussions
4. Measure for improvement
Will discuss our audit results more at the finish but one fine example of this is the QRP results I showed you
5. Engage front line staff
Engage front-line staff to take measures to keep healthcare environments safe and efficient. Productive ward. Patient safety first. QRP results
Competitive audits. Educators � policy changes also involve staff
6. Executive team support
Executive support � for the clinical educator team, background framework, competencies and practice development
TRANSITION STATEMENT � There are other practical tools and mechanisms in place that facilitated our introduction
Share Good practice/Recognition and Performance
Why does it work and what works? e.g. Learning from and within other teams (e.g. QRP, stop the clock/non essential tasks)
2. Take responsibility
e.g. Linked to acute competencies part of KSF
3. Learn from patients
e.g. key component of QRP. Incident reporting & action planning. Direct link to the CLIP report (complaints & litigation, incidents, PALS). Case discussions
4. Measure for improvement
Will discuss our audit results more at the finish but one fine example of this is the QRP results I showed you
5. Engage front line staff
Engage front-line staff to take measures to keep healthcare environments safe and efficient. Productive ward. Patient safety first. QRP results
Competitive audits. Educators � policy changes also involve staff
6. Executive team support
Executive support � for the clinical educator team, background framework, competencies and practice development
TRANSITION STATEMENT � There are other practical tools and mechanisms in place that facilitated our introduction
7. c. Other supportive mechanisms & tools:
24/7 Critical Care Outreach
Aggregate EWS/MEWS
EWS/NICE 50 Audits
Introduction of SBAR
SUI panel
Escalation policy
1: Coordinated & Supportive Strategy Has tended to be over reliance on outreach so where is the time for them to teach?
Aggregate scoring mechanism includes appropriate standards (e.g. Minimum obs, prescription of obs etc). Includes Maternity EWS
NICE 50 audit is huge single snapshot
SBAR is from NHS Institute
SUI and what we can learn (includes failure to rescue. Feeds back action plans and if necessary what can be learned for the whole Trust)
Escalation added into our policies:
If necessary, an individual can escalate concerns if they are not getting the required support, ultimately to the director of nursing or the medical director � this gives the right message to staff regarding the importance of not taking no for an answer. It empowers multi disciplinary staff to make the right decision at the right time so failure to rescue is minimised
So, moving onto our second main theme � what about the nuts and bolts of the competencies and is it worth doing them?Has tended to be over reliance on outreach so where is the time for them to teach?
Aggregate scoring mechanism includes appropriate standards (e.g. Minimum obs, prescription of obs etc). Includes Maternity EWS
NICE 50 audit is huge single snapshot
SBAR is from NHS Institute
SUI and what we can learn (includes failure to rescue. Feeds back action plans and if necessary what can be learned for the whole Trust)
Escalation added into our policies:
If necessary, an individual can escalate concerns if they are not getting the required support, ultimately to the director of nursing or the medical director � this gives the right message to staff regarding the importance of not taking no for an answer. It empowers multi disciplinary staff to make the right decision at the right time so failure to rescue is minimised
So, moving onto our second main theme � what about the nuts and bolts of the competencies and is it worth doing them?
8. Introduction
Before I talk about the advantages of competence I want to point out that we have real witnessed practical experience of how the advantages cited within the competency framework are real. For staff, it IS more than just jumping through hoopsMy team and I saw clear example of all of these as a direct consequence of our work
1. We can empower staff if competencies are supported by the right policies and processes.
They can help staff to be more assertive and confident
2. Helps inter-professional working
Sets clear pathways of responsibility (CG100 flyers � nursing vs doctor responsibility etc)
3. Enhance accountability
You know what is expected of you. Embedded within the competency documents which staff need to sign
4. Assist service planning, workforce development & role re-design
Adapted competencies are a result of and also influence Examples include Surgical close obs and stroke service who relied on us to support staff in these new areas
5. Adds to appraisals/clinical supervision/KSF
We have a lot of practical experience of this now and with staff who are at risk of �capability�
6. Integrates well with existing education & training
Not about re inventing the wheel (e.g. enhances preceptorship training & AP training)
Introduction
Before I talk about the advantages of competence I want to point out that we have real witnessed practical experience of how the advantages cited within the competency framework are real. For staff, it IS more than just jumping through hoopsMy team and I saw clear example of all of these as a direct consequence of our work
1. We can empower staff if competencies are supported by the right policies and processes.
They can help staff to be more assertive and confident
2. Helps inter-professional working
Sets clear pathways of responsibility (CG100 flyers � nursing vs doctor responsibility etc)
3. Enhance accountability
You know what is expected of you. Embedded within the competency documents which staff need to sign
4. Assist service planning, workforce development & role re-design
Adapted competencies are a result of and also influence Examples include Surgical close obs and stroke service who relied on us to support staff in these new areas
5. Adds to appraisals/clinical supervision/KSF
We have a lot of practical experience of this now and with staff who are at risk of �capability�
6. Integrates well with existing education & training
Not about re inventing the wheel (e.g. enhances preceptorship training & AP training)
9. Funds
5.5 WTE staff for a period of 2 years supported by research team (1 lead and 4.5 WTE team)
2. Clinical Educators
Practice based/peripatetic (more on this later)
3. NICE 50/NPSA
Competencies based on NICE 50, NPSA and NICE Competency framework
These acute competencies are for ALL staff caring for in patient adults
4. Aim at the outset for 90% target training
Staff caring for in patient adults is the target Funds
5.5 WTE staff for a period of 2 years supported by research team (1 lead and 4.5 WTE team)
2. Clinical Educators
Practice based/peripatetic (more on this later)
3. NICE 50/NPSA
Competencies based on NICE 50, NPSA and NICE Competency framework
These acute competencies are for ALL staff caring for in patient adults
4. Aim at the outset for 90% target training
Staff caring for in patient adults is the target
10. Point 1 � amended per discipline & area (talk about what a recorder does VS recogniser)
We limited focus on specific staff caring for in patient adults. This included OT�s, Physio, midwives, nursing staff and doctors. Having specifically amended competencies enabled each discipline and specialist area to �own� the competencies as they were more relevant and applicable. Who are recorders etc
Point 2 � KSF linked & mandatory (nursing staff, HCA and Midwives are done peri patetically)
The staff are made clear that they understand it is KSF linked � inability to complete interrupts ability to proceed on gateway. Immediately made mandatory once they are rolled out within a specific area and now delivered to staff on induction. Booklet for doctors
Point 3 � a word on primary and secondary responders � part of their foundation training (urgent stuff right at the start)
Primary Responder is mapped to Foundation level 1 competencies as is Secondary responder to Foundation level 2 (for the rest of the staff the competencies take the form of a booklet)
Point 4 � PT/OT teach selves
Physiotherapist and Occupational Therapist ward champions were trained to undertake training for their own staff with some support from us. Bulk of our work is with nurses, midwives and HCA
Point 5 � timing & penalty
Three months to complete from commencement
Commencement slip goes to training who then flag it on system until completion. First failure results in a reminder to ward manager and individual then some further time. Second failure results in a reminder to General manager, ward manager and individual and then slight further time given. Third failure results in reminder also sent to go Governance lead for immediate action
Point 1 � amended per discipline & area (talk about what a recorder does VS recogniser)
We limited focus on specific staff caring for in patient adults. This included OT�s, Physio, midwives, nursing staff and doctors. Having specifically amended competencies enabled each discipline and specialist area to �own� the competencies as they were more relevant and applicable. Who are recorders etc
Point 2 � KSF linked & mandatory (nursing staff, HCA and Midwives are done peri patetically)
The staff are made clear that they understand it is KSF linked � inability to complete interrupts ability to proceed on gateway. Immediately made mandatory once they are rolled out within a specific area and now delivered to staff on induction. Booklet for doctors
Point 3 � a word on primary and secondary responders � part of their foundation training (urgent stuff right at the start)
Primary Responder is mapped to Foundation level 1 competencies as is Secondary responder to Foundation level 2 (for the rest of the staff the competencies take the form of a booklet)
Point 4 � PT/OT teach selves
Physiotherapist and Occupational Therapist ward champions were trained to undertake training for their own staff with some support from us. Bulk of our work is with nurses, midwives and HCA
Point 5 � timing & penalty
Three months to complete from commencement
Commencement slip goes to training who then flag it on system until completion. First failure results in a reminder to ward manager and individual then some further time. Second failure results in a reminder to General manager, ward manager and individual and then slight further time given. Third failure results in reminder also sent to go Governance lead for immediate action
11. Point1 - Manager brief
Ward manager is seen several weeks before and during this interview (if necessary � PDSA):
Explanation of what is expected. List of key staff requested (at least 1 per 5 staff). Multiple copies of relevant competencies to be printed and an area to keep them safe (staff can mislay resulting in delay). Ward champions must be senior staff or sisters and must be free to mentor. We also point out as well as the competencies we will evidence specific training and exactly who we have delivered it to (e.g. Track & Trigger Training, Fluid balance, SBAR, ABCDE assessment, Emergency trolley, Escalation policy). If manager is not already we point out the link to the AIM course & NICE 50 competencies and when AIM courses are. Roughly two to three weeks per ward. We then ask manager if there is anything else we can help to train whilst we are at it. Manager doesn�t always brief staff so - we now tend to visit an area a few times. We were 24/7 but funding was an issue
Point 2 - Ward champions also:
Briefed as above & how to deal with staff who are not demonstrating competence. Also given hard copy and electronic resources
Point 3 - After the Visit
We do deal with serious issues there and then but we do delivering a post visit brief (using Pendleton�s rules of Feedback) which doesn�t just cover the competencies. It also includes feedback on issues relevant to the acutely ill patient (e.g. prioritisation of observations, handovers etc). Managers are set colour coded action plans
We did go back to several areas and there were three reasons. A - poor compliance so we had to re action plan and continue until we saw improvement. B - part of SUI planning/response. C � if the action plan (above) had serious concernsPoint1 - Manager brief
Ward manager is seen several weeks before and during this interview (if necessary � PDSA):
Explanation of what is expected. List of key staff requested (at least 1 per 5 staff). Multiple copies of relevant competencies to be printed and an area to keep them safe (staff can mislay resulting in delay). Ward champions must be senior staff or sisters and must be free to mentor. We also point out as well as the competencies we will evidence specific training and exactly who we have delivered it to (e.g. Track & Trigger Training, Fluid balance, SBAR, ABCDE assessment, Emergency trolley, Escalation policy). If manager is not already we point out the link to the AIM course & NICE 50 competencies and when AIM courses are. Roughly two to three weeks per ward. We then ask manager if there is anything else we can help to train whilst we are at it. Manager doesn�t always brief staff so - we now tend to visit an area a few times. We were 24/7 but funding was an issue
Point 2 - Ward champions also:
Briefed as above & how to deal with staff who are not demonstrating competence. Also given hard copy and electronic resources
Point 3 - After the Visit
We do deal with serious issues there and then but we do delivering a post visit brief (using Pendleton�s rules of Feedback) which doesn�t just cover the competencies. It also includes feedback on issues relevant to the acutely ill patient (e.g. prioritisation of observations, handovers etc). Managers are set colour coded action plans
We did go back to several areas and there were three reasons. A - poor compliance so we had to re action plan and continue until we saw improvement. B - part of SUI planning/response. C � if the action plan (above) had serious concerns
12. Developing and assessing competence in clinical practice is a challenge
Witnessing the reality of practice
Keeping back � observing. If competent you simply sign off. You get to see practical improvements in real time (e.g. FB)
Link cause & effect
Ideal for promoting IPE (e.g. EWS � ABCDE � skills drills)
Stop the clock for observations came in as a result of linking cause & effect (e.g. Delayed obs)
Thinking about underpinning theory or logic (ritualistic practice e.g. bed baths more important than obs)
Thinking about why or how things happen the way they do (why have you sent that HCA to scan with that patient who has chest pain?)
Giving feedback
Pendleton�s rules of effective feedback (both for individual clinicians and managers)
Facilitating where you can (e.g. Tell me more about this patient � what�s missing?)
Educating where you see the need but knowing where to step in and lead by example especially if there are safety issues.
Visual teaching aids/laminates and practice improvements all support our practice presence
Developing and assessing competence in clinical practice is a challenge
Witnessing the reality of practice
Keeping back � observing. If competent you simply sign off. You get to see practical improvements in real time (e.g. FB)
Link cause & effect
Ideal for promoting IPE (e.g. EWS � ABCDE � skills drills)
Stop the clock for observations came in as a result of linking cause & effect (e.g. Delayed obs)
Thinking about underpinning theory or logic (ritualistic practice e.g. bed baths more important than obs)
Thinking about why or how things happen the way they do (why have you sent that HCA to scan with that patient who has chest pain?)
Giving feedback
Pendleton�s rules of effective feedback (both for individual clinicians and managers)
Facilitating where you can (e.g. Tell me more about this patient � what�s missing?)
Educating where you see the need but knowing where to step in and lead by example especially if there are safety issues.
Visual teaching aids/laminates and practice improvements all support our practice presence
13. Peripatetic approach is not just about the bedside but is about other aspects of practice and whether or not they promote safe care of acutely unwell patients
Point 1 - Observation of handover and communication (give direct feedback on handover by both docs & nurses)
Pendlteton�s rules of constructive feedback also relates to these important processes as well as direct clinical practice
The peripatetic approach helps to empower staff as it is grounded in the real world. What we suggest for practice improvement has to be seen to be realistic and achievable.
These two pointers have led to a number of practice improvements that we had to lead on (will discuss shortly)
Point 2 � Prioritisation and organisation (e.g. drugs round. I ward does all drugs � CD�s and kardex together, another does them seperately e.g. do the main drugs then do a second CD round)
There can be difficulties
Peripatetic approach is not just about the bedside but is about other aspects of practice and whether or not they promote safe care of acutely unwell patients
Point 1 - Observation of handover and communication (give direct feedback on handover by both docs & nurses)
Pendlteton�s rules of constructive feedback also relates to these important processes as well as direct clinical practice
The peripatetic approach helps to empower staff as it is grounded in the real world. What we suggest for practice improvement has to be seen to be realistic and achievable.
These two pointers have led to a number of practice improvements that we had to lead on (will discuss shortly)
Point 2 � Prioritisation and organisation (e.g. drugs round. I ward does all drugs � CD�s and kardex together, another does them seperately e.g. do the main drugs then do a second CD round)
There can be difficulties
14. Peripatetic approach is useful but not without its challenges. Developing ward champions is a key tactic and you should ensure AIM course is mandatory if not for all staff then certainly at least for ward champions. Build relationships early
Point 1 � Witnessing issues
Witnessing questionable practice/clinical incidents takes tact and where Pendleton�s rules comes in. A sound knowledge base for educators is essential as well as the need to facilitate appropriate support & de brief. On a different note � the witnessing of competency acquisition is sometimes difficult � this is when you can utilise scenarios. Skills drills can be useful but are of very limited use in a busy clinical area, (seeing competencies)
Point 2 & 3 � Time Demands/Pressure on staff/Dealing with meltdown
If a member of staff is stressed or does not have time � deal with it carefully and know when to back off. If a ward is in meltdown you can offer relevant strategic help and advice but sometimes its best to focus elsewhere and come back but revise your input strategy
Point 4- Communication � does improve as a result of our input
Sometimes reception can be frosty, in all cases this has been when management have been tardy in involving their staff in what we are there for. Now we recognise the need to check areas before you start despite manager prep. Staff are acceptably cautious at first usually but in most cases once they realise why we are there they tend to relax into the process. In some cases, (as we will see � we have been able to assist practice development and make their lives easier in the bargain)
Important last point
Staff can mislay their competencies. They are told at the outset that they are responsible for them and no one else
Peripatetic approach is useful but not without its challenges. Developing ward champions is a key tactic and you should ensure AIM course is mandatory if not for all staff then certainly at least for ward champions. Build relationships early
Point 1 � Witnessing issues
Witnessing questionable practice/clinical incidents takes tact and where Pendleton�s rules comes in. A sound knowledge base for educators is essential as well as the need to facilitate appropriate support & de brief. On a different note � the witnessing of competency acquisition is sometimes difficult � this is when you can utilise scenarios. Skills drills can be useful but are of very limited use in a busy clinical area, (seeing competencies)
Point 2 & 3 � Time Demands/Pressure on staff/Dealing with meltdown
If a member of staff is stressed or does not have time � deal with it carefully and know when to back off. If a ward is in meltdown you can offer relevant strategic help and advice but sometimes its best to focus elsewhere and come back but revise your input strategy
Point 4- Communication � does improve as a result of our input
Sometimes reception can be frosty, in all cases this has been when management have been tardy in involving their staff in what we are there for. Now we recognise the need to check areas before you start despite manager prep. Staff are acceptably cautious at first usually but in most cases once they realise why we are there they tend to relax into the process. In some cases, (as we will see � we have been able to assist practice development and make their lives easier in the bargain)
Important last point
Staff can mislay their competencies. They are told at the outset that they are responsible for them and no one else
15. Point 1 � AIM 9you can always tell who has done an AIM course)
AIM course is NHS North West
Due to our input AIM course is now held 2-4 times per month and is now a formal part of our approach to management of a patient triggering EWS
Point 2 - HCA
All HCA staff in the Trust must now also evidence they have attended specific Trust training on observations
Point 3 � Bank/Agency
We identified and responded to the risk here. All bank staff must have received training on observations. Key members of our local staff agency were trained in what we expected and all of agency staff have now received formal training on our charts and how they are used
Point 4 - Audit
We audit wards post SUI daily whilst we are there to determine immediate improvements as well as routine audits
Let�s look at some of the practice development we did as additional frame-working for our competenciesPoint 1 � AIM 9you can always tell who has done an AIM course)
AIM course is NHS North West
Due to our input AIM course is now held 2-4 times per month and is now a formal part of our approach to management of a patient triggering EWS
Point 2 - HCA
All HCA staff in the Trust must now also evidence they have attended specific Trust training on observations
Point 3 � Bank/Agency
We identified and responded to the risk here. All bank staff must have received training on observations. Key members of our local staff agency were trained in what we expected and all of agency staff have now received formal training on our charts and how they are used
Point 4 - Audit
We audit wards post SUI daily whilst we are there to determine immediate improvements as well as routine audits
Let�s look at some of the practice development we did as additional frame-working for our competencies
16. 3. Competence & Practice Development Introduction
Competencies must be based on practical, realistic and supportive policies and guidelines influenced from the ground floor up. The degree of work needed to ensure this was wholly unanticipated at the outset of the project. We would have limited success if we did not deal with practice development issues that were barriers to the success of the competencies.
Point 1 - Policies guidelines
Example - fluid balance policy & observations policies now exist which contains realistic and achievable guidance on how to improve practice (e.g. estimating). When to start/stop FB, links to obs guidelines, hydration policy, policy for acute illness
Point 2 - Staff involvement & ownership
Much of our CG100 observations policy has emerged from the ground floor up. People must see the practical �worth�. This is part of the process of planning for any and all barriers to success
Point 3 - Barriers to success accessing the correct Trust mechanisms for making change and getting the right senior champions & exec team
Point 4 - Personal responsibility versus Trust responsibility
Roles and responsibilities are made very clear in the relevant policies (e.g. observations and fluid balance) and competencies, (signing for training, FB entries, competencies etc). We work through our existing ward processes (e.g. NPSG and NPPG) to ensure high level staff as well as ground level staff are engaged in practice development.
Stronger link between competency � guideline - clinical practice
Point 5 � Audits & feeding back
Feeding back our successes and positive witnessing of good practice is itself empowering. We have taken great measures to ensure that particularly good practice areas are highlighted by the Trust
Introduction
Competencies must be based on practical, realistic and supportive policies and guidelines influenced from the ground floor up. The degree of work needed to ensure this was wholly unanticipated at the outset of the project. We would have limited success if we did not deal with practice development issues that were barriers to the success of the competencies.
Point 1 - Policies guidelines
Example - fluid balance policy & observations policies now exist which contains realistic and achievable guidance on how to improve practice (e.g. estimating). When to start/stop FB, links to obs guidelines, hydration policy, policy for acute illness
Point 2 - Staff involvement & ownership
Much of our CG100 observations policy has emerged from the ground floor up. People must see the practical �worth�. This is part of the process of planning for any and all barriers to success
Point 3 - Barriers to success accessing the correct Trust mechanisms for making change and getting the right senior champions & exec team
Point 4 - Personal responsibility versus Trust responsibility
Roles and responsibilities are made very clear in the relevant policies (e.g. observations and fluid balance) and competencies, (signing for training, FB entries, competencies etc). We work through our existing ward processes (e.g. NPSG and NPPG) to ensure high level staff as well as ground level staff are engaged in practice development.
Stronger link between competency � guideline - clinical practice
Point 5 � Audits & feeding back
Feeding back our successes and positive witnessing of good practice is itself empowering. We have taken great measures to ensure that particularly good practice areas are highlighted by the Trust
17. 3. Competence & Practice Development Point 1 - There was no clear Trust Wide Policy on Oxygen therapy
Point 2 � Prioritisation tool & stop the clock
Staff had no clear practical guidance on why and how to prioritise the clinical observation of patients. This is where stop the clock and the prioritisation tool came in. Stop the clock- this was developed initially by nursing staff on orthopaedic wards following incidents of clearly documented deterioration with no action documented�.. and was subsequently picked up by medical wards. There are set times with clear prioritisation
Point 4 � EWS & ABCDE aim assessment
EWS raised 0-5 and patient not in extremis? Perform ABCDE assessment then repeat EWS, if EWS> perform as graded response dictates
Point 5 � Handover communication
Handovers for acutely ill now include: EWS, fluid balance, details of referral and management plan
Point 1 - There was no clear Trust Wide Policy on Oxygen therapy
Point 2 � Prioritisation tool & stop the clock
Staff had no clear practical guidance on why and how to prioritise the clinical observation of patients. This is where stop the clock and the prioritisation tool came in. Stop the clock- this was developed initially by nursing staff on orthopaedic wards following incidents of clearly documented deterioration with no action documented�.. and was subsequently picked up by medical wards. There are set times with clear prioritisation
Point 4 � EWS & ABCDE aim assessment
EWS raised 0-5 and patient not in extremis? Perform ABCDE assessment then repeat EWS, if EWS> perform as graded response dictates
Point 5 � Handover communication
Handovers for acutely ill now include: EWS, fluid balance, details of referral and management plan
18. 3. Competence & Practice Development Point 1 � Reducing EWS
Until recently only F2 or Band 6 (Sister) could reduce observations frequency). Now there are flow charts for areas of exception using EWS � so that they can delay referral or if appropriate de-escalate EWS frequency as long as EWS is < trigger point and patient is of no concern
Point 2 � New areas (assist in development of new areas such as surgical close obs/stroke)
Point 3 � Uncommon clinical competencies
Competency crib sheets and bullet point sheets, (e.g one or two sided bullet point sheets that can be accessed if staff come across a chest drain, tracheostomy or CVP etc). Just enough information to allow for the patient to be �safe� until further expertise can be accessed. What makes me safe?
Point 4 � EWS application universal
A&E didn�t initially use EWS which we identified as an opportunity for a patient to deteriorate (wards and A&E were speaking in different languages). Now EWS is used in A&E and always checked prior to transfer � further reducing opportunity for a missed opportunity to spot a potential problem.
Obstetrics now have MEWS and EWS is even used in recovery and daycase (with exception/flow charts etc)
Point 5 � Ward Feedback & change Our feedback has changed practice
In one ward our feedback has triggered a staffing review, in another area one area was split into two wards to help it run more efficiently. We also influenced a temporary reduction in capacity in one area until processes could be reviewed
Point 6 � Skills Drills (starting to run in our acute respiratory ward)
Point 1 � Reducing EWS
Until recently only F2 or Band 6 (Sister) could reduce observations frequency). Now there are flow charts for areas of exception using EWS � so that they can delay referral or if appropriate de-escalate EWS frequency as long as EWS is < trigger point and patient is of no concern
Point 2 � New areas (assist in development of new areas such as surgical close obs/stroke)
Point 3 � Uncommon clinical competencies
Competency crib sheets and bullet point sheets, (e.g one or two sided bullet point sheets that can be accessed if staff come across a chest drain, tracheostomy or CVP etc). Just enough information to allow for the patient to be �safe� until further expertise can be accessed. What makes me safe?
Point 4 � EWS application universal
A&E didn�t initially use EWS which we identified as an opportunity for a patient to deteriorate (wards and A&E were speaking in different languages). Now EWS is used in A&E and always checked prior to transfer � further reducing opportunity for a missed opportunity to spot a potential problem.
Obstetrics now have MEWS and EWS is even used in recovery and daycase (with exception/flow charts etc)
Point 5 � Ward Feedback & change Our feedback has changed practice
In one ward our feedback has triggered a staffing review, in another area one area was split into two wards to help it run more efficiently. We also influenced a temporary reduction in capacity in one area until processes could be reviewed
Point 6 � Skills Drills (starting to run in our acute respiratory ward)
19. 4. Results We have received notable recognition for our work
Point 1 � In addition:
Subjective responses � positive feedback from ward staff and managers
Good feedback from exec teams, Trust education & training group, steering group for acute illness and resuscitation team
Point 2: Results feedback:
Our Trust results are communicated to staff through:
Clinical Governance
ACE committee
Directly via Senior Clinical Nurses to ward staff
Waiting for our research teams findings but in the meantime�.We have received notable recognition for our work
Point 1 � In addition:
Subjective responses � positive feedback from ward staff and managers
Good feedback from exec teams, Trust education & training group, steering group for acute illness and resuscitation team
Point 2: Results feedback:
Our Trust results are communicated to staff through:
Clinical Governance
ACE committee
Directly via Senior Clinical Nurses to ward staff
Waiting for our research teams findings but in the meantime�.
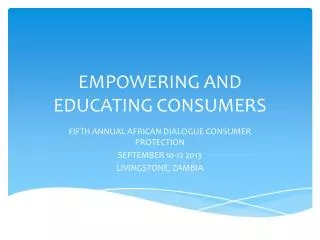
20. EWS Audit Trust Wide 2009
21. This and the next slide presents data that was part of our NICE 50 audit � note the radical improvement
Dates: March 2008, October 2008, May 2009, November 2009
The percentage doesn�t mean EWS has never been done. It simply means that if EWS has been missed more than once in 24 hours the audit criteria have not been met. This and the next slide presents data that was part of our NICE 50 audit � note the radical improvement
Dates: March 2008, October 2008, May 2009, November 2009
The percentage doesn�t mean EWS has never been done. It simply means that if EWS has been missed more than once in 24 hours the audit criteria have not been met.
22. Here is another one from the NICE 50...
Again, this doesn�t means observations have not been recorded or increased appropriately. It just means that the prescription for observations and their frequency has not been documentedHere is another one from the NICE 50...
Again, this doesn�t means observations have not been recorded or increased appropriately. It just means that the prescription for observations and their frequency has not been documented
23. Points to explain:
- We will achieve around 60% as opposed to the original 90%.
- This reflects the sheer amount of practice development and support necessary which was totally unanticipated
- If we had JUST focused on the competencies alone we may have achieved higher.
- However, we would have been paying lip service to the competencies.
- We feel patients are safer with 52% completion
Figures relevant up until mid March 2010
Primary Responders � Outreach and Specialist Nurses � competencies have been drawn up but not launched for these groups yet
Secondary responders � this will also shortly include ST and middle grades
Difficulties keeping the data live as staff leave and start all the time, every quarter these figures are re-verified to take account of this
There are only three clinical areas left for us to complete � recovery, short stay and haematology
74% of the relevant workforce engaged in training! 59% or more will be throughPoints to explain:
- We will achieve around 60% as opposed to the original 90%.
- This reflects the sheer amount of practice development and support necessary which was totally unanticipated
- If we had JUST focused on the competencies alone we may have achieved higher.
- However, we would have been paying lip service to the competencies.
- We feel patients are safer with 52% completion
Figures relevant up until mid March 2010
Primary Responders � Outreach and Specialist Nurses � competencies have been drawn up but not launched for these groups yet
Secondary responders � this will also shortly include ST and middle grades
Difficulties keeping the data live as staff leave and start all the time, every quarter these figures are re-verified to take account of this
There are only three clinical areas left for us to complete � recovery, short stay and haematology
74% of the relevant workforce engaged in training! 59% or more will be through
24. 100 represents average mortality across the country
Does anyone remember mortality? Do you know what your mortality rate is in your Trust?
Ours back in August 2008 was 136 (before re coding of the data set it was 108)
Each slide (confidence interval) of relative risk has complex rare procedures of high risk and poor outcome at the top end and very routine low risk at the bottom � this is why the middle bit is the mean
Median range of the sample groups has improved and we are now well below the target range for relative risk reduction (82%) which puts us in the top 25% of Trusts
THIS REFLECTS combination of all of our Trust mechanisms of which we formed a major role100 represents average mortality across the country
Does anyone remember mortality? Do you know what your mortality rate is in your Trust?
Ours back in August 2008 was 136 (before re coding of the data set it was 108)
Each slide (confidence interval) of relative risk has complex rare procedures of high risk and poor outcome at the top end and very routine low risk at the bottom � this is why the middle bit is the mean
Median range of the sample groups has improved and we are now well below the target range for relative risk reduction (82%) which puts us in the top 25% of Trusts
THIS REFLECTS combination of all of our Trust mechanisms of which we formed a major role
25. Mortality Although as stated earlier we changed the data set, regardless of the data set we still showed a drop in 15%
We set an ambitious goal to reduce mortality by 15% in one year � we achieved this and have continued to reduce mortality � for the last 2-months we have been within the 25% Trusts nationally for mortality (Dr Foster)
In the last few months this translates as 73 people less dying. 73 people who would not have gone home
The bottom line shows the older data set and the top shows the new data set
Although as stated earlier we changed the data set, regardless of the data set we still showed a drop in 15%
We set an ambitious goal to reduce mortality by 15% in one year � we achieved this and have continued to reduce mortality � for the last 2-months we have been within the 25% Trusts nationally for mortality (Dr Foster)
In the last few months this translates as 73 people less dying. 73 people who would not have gone home
The bottom line shows the older data set and the top shows the new data set
26. Questions� You need to work FAST and communicate WIDELY and inclusively. Let your champions do the work for you
Reliance on competency acquisition in absence of supportive practice development and a Trust Wide Strategy is bound to have limitations
Staff loss requires regular consolidation. Ultimately, ward staff will get better at replacing their key ward champions but was difficult to start with
Either a feedback action plan has major concerns or SUI occurs � in either case this usually merits revisit
Extra care must be taken to ensure that key content is delivered in the right place at the right time for foundation doctors and this is something we are still working on
Practice development can be both good and bad as it can create short term confusion (the pace of change is rapid � as in chart changes etc). However, in the long term it garners better staff compliance and respect as staff feel better engaged (after all � the changes have come from them)
Changes advised by peripatetic educators can be seen to reflect the realism of practice and the needs of staff whilst also serving to increase patient quality and safety. In this way, peripatetic educators empower front line staffYou need to work FAST and communicate WIDELY and inclusively. Let your champions do the work for you
Reliance on competency acquisition in absence of supportive practice development and a Trust Wide Strategy is bound to have limitations
Staff loss requires regular consolidation. Ultimately, ward staff will get better at replacing their key ward champions but was difficult to start with
Either a feedback action plan has major concerns or SUI occurs � in either case this usually merits revisit
Extra care must be taken to ensure that key content is delivered in the right place at the right time for foundation doctors and this is something we are still working on
Practice development can be both good and bad as it can create short term confusion (the pace of change is rapid � as in chart changes etc). However, in the long term it garners better staff compliance and respect as staff feel better engaged (after all � the changes have come from them)
Changes advised by peripatetic educators can be seen to reflect the realism of practice and the needs of staff whilst also serving to increase patient quality and safety. In this way, peripatetic educators empower front line staff