Download
1 / 36
460 likes | 1.48k Views
Review for Provider Reappointments. Coding and Compliance. Course Objectives. The purpose of this course and its follow-on test is to provide physicians and other clinicians, who are being re-credentialed by UNC Hospitals, with important information on three issues…. Course Objectives.

E N D
Review for Provider Reappointments Coding and Compliance
Course Objectives The purpose of this course and its follow-on test is to provide physicians and other clinicians, who are being re-credentialed by UNC Hospitals, with important information on three issues…
Course Objectives • Why coding and compliance is important to you and your practice • Keys to correctly coding hospital and office visits - Evaluation and Management (E&M) Services • Teaching physician (TP) rules. In order to bill for services when working with residents and fellows, the teaching physician must abide by federal and state laws and regulations
Why coding and complianceis important to you and your practice
Reimbursement • Doing only what is medically necessary • Documenting what you do • Billing what you document Providing good care while billing accurately and confidently requires: Understanding and applying coding and compliance conventions can improve the level of reimbursement for UNC P&A practices as well as the quality of the medical record documentation.
Why Compliance Good documentation and billing practices make for good patient care Recovery Audit Contractors (RACS)—Medicare and Medicaid Office of Inspector General (OIG), Health & Human Services Routine error rate testing and auditing programs
Why Compliance • Residents are paid through the hospital by Part A Medicare. Medicare pays a portion of the residents’ salaries based on the proportionate share of Medicare at the teaching hospital. • Teaching physicians are paid by Part B Medicare on a fee-for-service basis. • The government, through Medicare, will pay for both resident and TP services if both participate. If the TP does not participate in a given patient service, the TP cannot bill.
Why Compliance Two problems have caused a majority of refunds and penalties: • The TP billed and he/she may have been present and participated in the care, but TP presence was not documented. • The documentation did not support the level of evaluation and management (E&M) service billed. The billed level of service may have been provided, but it was not documented.
Keys to correctly coding hospital and office visits - Evaluation and Management (E&M) Services
Choose the Outpatient Category • Outpatient E&M Categories • Consultation • New • Established
Use of Consultation Codes • Use when expert opinion or advice is requested by an appropriate source involved in that patient’s care • Does not include patients “referred for management of a condition” or self-referred • Use outpatient consultation codes only one time per request, subsequent visits are established patient visits • A consulting physician may initiate diagnostic and/or therapeutic services at the same visit and the initial visit remains a consultation • Written or verbal request must be documented in the rendering physician’s note and the consultant’s opinion communicated by written report to the requesting physician
Documenting Consultations Documentation of a consultation request must be clearly stated in the note: WRONG: Mr. Patient referred by Dr. Jones for management of GERD symptoms. RIGHT: “Mr. Patient is seen in consultation at the request of Dr. Jones for evaluation of abdominal pain.” Please be sure to document that a copy of the note (cc: Dr. Jones) is to be sent to the requesting physician.
New Patient • Has not received any professional evaluation and management (E&M) services from the physician or another physician of the same specialty who belongs to the same group practice within the past three years, including inpatient, outpatient or emergency room. • A patient would still be considered “new” if a diagnostic procedure was billed without an E&M visit charge.
Established Patient • Has received an E&M service from the division within the past three years including inpatient, emergency room or inpatient or outpatient consultations
Visit Components Consults and new patient visits must include all three of the following components – established patient visits must include any two of the three: • History • History of present illness Documenting History • Review of systems History example • Past family and social history • Physical examination 1995 Physical Exam 1997 Single Organ Exams • Medical decision Making • Diagnosis and management options Documenting MDM • Amount and complexity of data reviewed • Overall risk Risk Table Click these links for more information
Visit Levels • Billing at a higher level than actually provided and documented is one of the two chief issues contributing to CMS fraud allegation settlements • The laminated, pocket-sized physician’s coding card is a valuable guide to correct coding. To request a copy of this card please call 843-8638. • Questions on correct coding and compliance issues should be directed to either of the Compliance Auditors at 843-8638. • Click on this link fordocumentation requirements at various E&M levels of service.
Visit levels – based on time • Document the total time of the visit. • Over 50 % of an outpatient visit must be spent in face-to-face counseling and treatment planning and so documented. For Medicare patients, count only face time between the Teaching Physician and the patient. • For inpatient count total for the day of counseling, coordination of care and time on floor in care of the patient.
Visit levels – based on time (con’t) • The note must include a description of the counseling and treatment planning. • The physician’s coding card contains minimum time requirements for each visit level. • Note that the minimum times are different for each of the three categories of visits: consults, new patient and established patient. • Click on this link for additional time-based billing information.
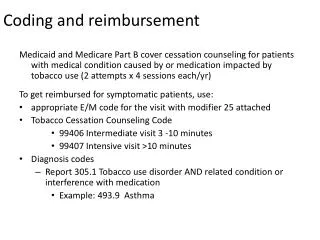
Modifier 25 • Append a modifier 25 to an E&M code if a significant, separately identifiable E&M service is performed by the same physician on the same day of a procedure or other service. • The patient’s condition must require E&M services above and beyond what would normally be performed in the provision of the procedure. • The necessity for the E&M service may be prompted by the same diagnosis as the procedure. • A new patient E&M service is considered separate from the same day surgery or procedure—no 25 modifier needed.
Modifier 25 • For an established patient, if the E&M service resulted in the initial decision to perform a minor procedure (0-10 days global period) on the same day and medical necessity indicates an E&M service beyond what is considered normal protocol for the procedure, the 25 modifier is appropriate. • To determine the correct level of E&M service to submit, identify services unrelated to the procedure and use as E&M elements. • Clearly mark the encounter form to indicate that a 25 modifier should be attached to the E&M.
3. Teaching physician (TP) rules—supervision of residents and billing Medicare and Medicaid
Medicare TP Attestation Requirement • The 11/22/02 revisions to the regulations provide that, for E&M services, the TP does not have to duplicate any resident documentation. • The TP must be present during the key portions of the service and personally document his or her presence. • The resident note alone, the TP note alone or a combination of the two may be used to support the level of service billed. • Documentation by a resident of the presence and participation of the TP is not sufficient. • Documentation may be dictated and typed, hand-written or a computer statement initiated by the TP.
Medicare’s Examples of Unacceptable TP notes • "Agree with above." followed by legible countersignature or identity; • "Rounded, Reviewed, Agree." followed by legible countersignature or identity; • "Discussed with resident. Agree." followed by legible countersignature or identity; • "Seen and agree." followed by legible countersignature or identity; • "Patient seen and evaluated." followed by legible countersignature or identity; and • A legible countersignature or identity alone. The preceding six and similar statements don’t make it possible to determine whether the TP was present, evaluated the patient, and/or had any involvement with the plan of care.
Medicare Exception for Primary Care • CMS does not require direct patient contact for primary care, lower-level visits provided by residents with more than six months training working in approved primary care programs. • Approved primary care centers at UNC: • Family Medicine • General Medicine • General Pediatrics • Women’s Primary Health
Medicare Primary Care Exception • TP may supervise up to 4 residents on immediately available basis • Residents must have completed 6 months training • TP must review each patient case w/resident during or right after visit • TP must document his/her contemporaneous discussion of the patient’s condition with the resident. • Only E&M codes 99201-03, 99211-13 may be billed • TP may see and evaluate a patient in a primary care exception clinic and bill a higher level of service
Medicare Supervision Guidelines for Procedures Performed with Residents • TP must be present during critical and key portions & immediately available throughout surgical procedures and endoscopic operations: • TP decides what portions are key • If present entire time, the resident’s note can attest to that • If present for key portions only, TP must document extent of involvement • Two overlapping surgeries: • Key portions must happen at different times • Must be available to return to either
Medicare Supervision Guidelines for Procedures Performed with Residents • Minor procedures of<5 minutes • Must be present the entire time • Endoscopies (other than surgical operations) • TP must be present for entire viewing including insertion and removal
Medicare Supervision Guidelines for Supervision of Specific Procedures • Radiology/Diagnostic Tests • Image and resident interpretation must be reviewed by TP to be billable • TP may sign acknowledging agreement or edit, co-signature insufficient • Psychiatry • TP presence requirement met by concurrent observation of the service by video or one-way mirror • Must be present for entire period of time billed if time-based psychotherapy code is used
Medicare Supervision Guidelines for Specific Procedures • Time-based procedures billed on TP time only • Critical care • Hospital discharge day management • Prolonged services • Care plan oversight • E&M counseling/coordination of care • Specific complex or high-risk procedures require continual personal TP supervision • Interventional radiologic/cardiologic codes • Cardiac cath, stress tests, transesophageal ekg
Medicaid Requirements Medicaid requires that the TP be "immediately available" to the resident and patient and use "direct supervision" for procedures. Direct supervision does not necessarily mean that the TP must be present in the room when the service is performed. The degree of supervision is the responsibility of the TP and is based on the skill, level of training and experience of the resident as well as the complexity and severity of the patient's condition. Written documentation in the medical record for Medicaid patients must clearly designate the supervising physician and be signed by that physician.
The Hospitals’ financial health is important to you Only physicians can make a decision to admit as an inpatient, place in observation status or extended recovery. Only physicians can change the patient status. Clinical Care Management (CCM) staff assist in determining the appropriate status. Short stays have been a recent focus of government auditors and large refunds have been required due to documentation of medical necessity for an inpatient admission • Leaving patients in observation who should be admitted results in lost revenue to UNC Hospitals.
You can identify the outpatients on your census Billing Status OBS (16) OBS (28) EXR (6) EXR will always be red, as it is an unbillable status. OBS Appears green until 12 hrs Appears yellow from 13-20 hrs Appears red from 21 hours onward Think: when the field is red, we’re in the red
Eliminating Confusion (and Revenue Loss) Problems with the “Admit” word • Interpreted as inpatient intent to CMS • Means “Place Patient in Bed” at UNCH • Does not define a billing status • Generally causes confusion • Can cause CMS retractions Avoid an order contradiction in notes • “Will admit to Obs” • “Will place on Inpatient Observation”
The Importance of the H&P • Admitting team documentation required for billing status determination • Inpatient medical necessity is established by a review of criteria and documented intent/risk by the admitting team • Billing status begins when the order is placed Delay in H&P or admit note with intent Delay in Billing Status Order Un-billable days = =
Where To Get Help • www.med.unc.edu/compliance/ • UNC P&A Professional Charges (code inpatient services and some outpatient procedures) 962-8391 • School of Medicine Compliance Office 843-8638 • Heather Scott, CPC, Compliance Officer • Keishonna Carter, CPC, Compliance Review Analyst • Nirmal Gulati, CPC, Compliance Auditor • Lateefah Ruff, Office Assistant • Confidential Help Line 800-362-2921 • AMA CPT Manual